“Window of Tolerance” is a term originally coined by Dr. Dan Siegel commonly used to understand and describe normal brain/body reactions, especially following adversity.
It is also a term used to describe the zone of arousal in which a person is able to function most effectively.
Essentially, the size of our ‘window’ depends upon how much we are able to tolerate mild fluctuations in mood, energy levels, and the challenges and demands of life, whilst remaining in the Optimal Zone.
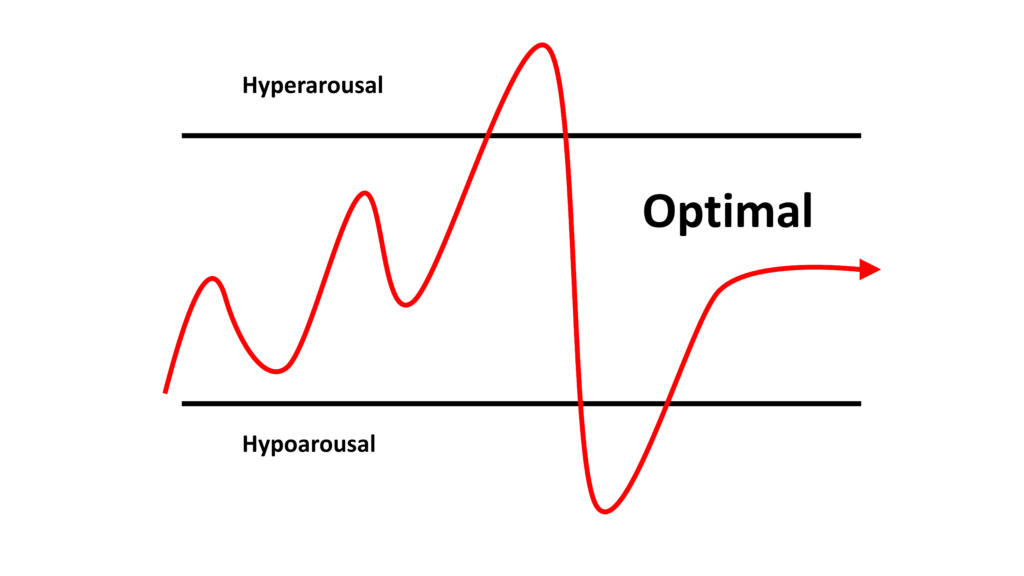
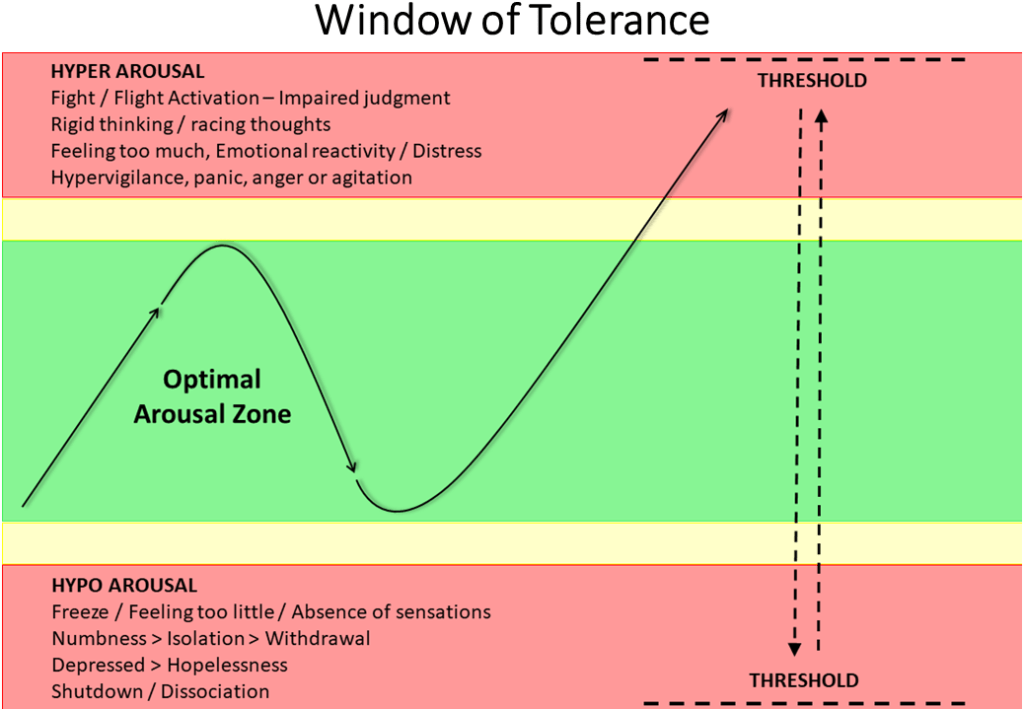
As seen in the diagram below, there is an Optimal Zone (or range) that we can function.
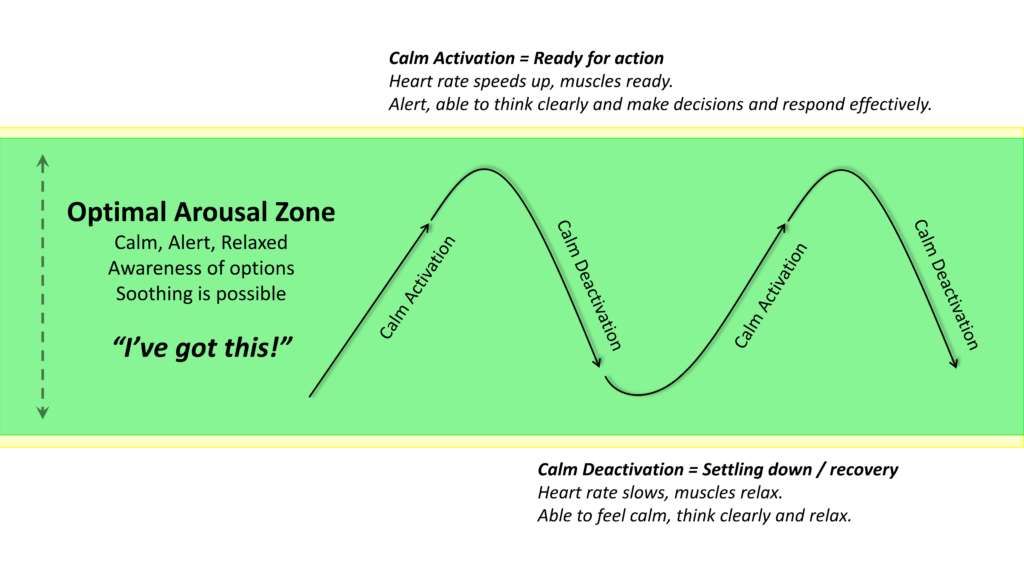
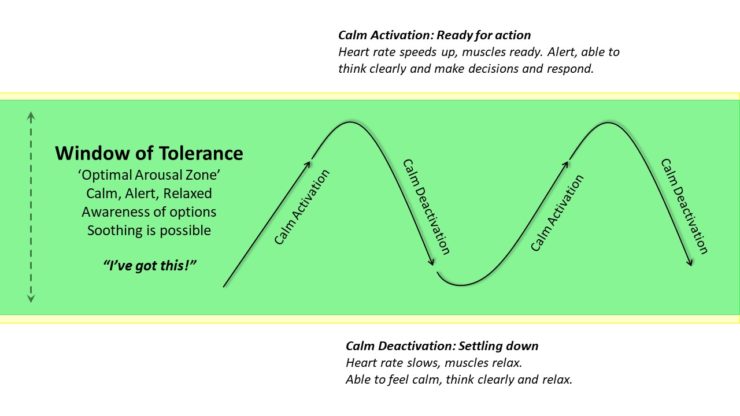
The Optimal Zone: Calm Activation & Deactivation
When we are within our Window of Tolerance we are essentially in the optimal zone (depicted above), our nervous systems (Sympathetic and Parasympathetic) are in a state of balance, which allows for adaptive responses to stress (i.e., Calm Activation depicted above) and a capacity for emotional regulation to balance this stress (i.e., Calm Deactivation, depicted above). In other words, we are calm but alert enough to be engaged in what we are doing without it being excessive, and we have ‘headroom’ to manage (and recover from) any challenges that may arise. Thus, when we are within our Window of Tolerance, we can engage in flexible thinking, effective communication and actions, and we are able to cope with daily stressors, build healthy relationships, and regulate our emotions constructively as required.
Just like how a thermostat in an air-conditioner makes micro-adjustments to temperature to keep it within a comfortable range, staying within the Optimal range of our Window of Tolerance requires awareness and skills, so that we can attend to our needs and can regulate our arousal level to match the situation at hand. Ordinarily we can do this either with self-soothing actions (or by reaching out to trusted soothing others) when we need to Deactivate our arousal, or via safe, healthy activities that stimulate us when we need to Activate our arousal.
However, the accumulation of Stress and/or feeling a state of Threat can shrink our Window of Tolerance. Once pushed outside our Window of Tolerance, it can become very difficult to take in new information. This is because these states of Hyper-arousal and Hypo-arousal are ancient physiological survival mechanisms that are shared across species throughout the entire animal kingdom.
For people who have experienced significantstress (which may either be the result of a single incident, or ‘toxic stress’ resulting from the accumulation of triggering events), it is common for the brain to become ‘stuck’ in high levels of Activation or Deactivation – and this can either lead to an inability to stay calm (triggering the fight / flight response) or shutting down (the freeze response) involuntarily when confronted with stress.
In other words, a threat, or the accumulation of excessive stress, or traumatic experiences can disrupt an individual’s ability to stay within their Window of Tolerance, causing them to become overwhelmed or shut down.
For example, if someone becomes hyperaroused, they may exhibit symptoms of anxiety, anger, or panic. On the other hand, if they become hypoaroused, they might experience symptoms of depression, dissociation, or a sense of detachment. As will be discussed, this is not the fault of the individual – it is simply how our brain’s became wired (i.e., evolved to protect us).
Understanding the Window of Tolerance is crucial in the context of therapy. For instance, a major initial aim in preparation for trauma therapies (such as EMDR Therapy) is often to help individuals expand their Window of Tolerance by developing skills for emotional regulation and increasing their capacity to tolerate distress. This work commonly includes cultivating mindfulness, self-awareness, and self-compassion to maintain a balanced state, which increases our capacity to remain within our Window of Tolerance. By developing these skills, individuals can enhance their resilience, improve their emotional well-being, and navigate life’s challenges more effectively. These same skills are highly useful in the ‘treatment phase’ of trauma therapies and help to make an individual’s experience of healing, safer and more manageable.
Even for those of us who have not experienced significant trauma, if we simply lack awareness – or have underdeveloped self-regulation skills – we may also become either too aroused(hyper-arousal) or we may completely shut down (hypo-arousal) when we encounter threats or stress. (Note: We also may not have been taught good self-care strategies and so the actions we take to reduce stress may be inadvertently contributing to the problem.)
The Window of Tolerance represents the ideal middle ground between these extremes. When we are within our Window of Tolerance, we are in a state of balance, allowing for adaptive responses to stressors and emotional regulation.
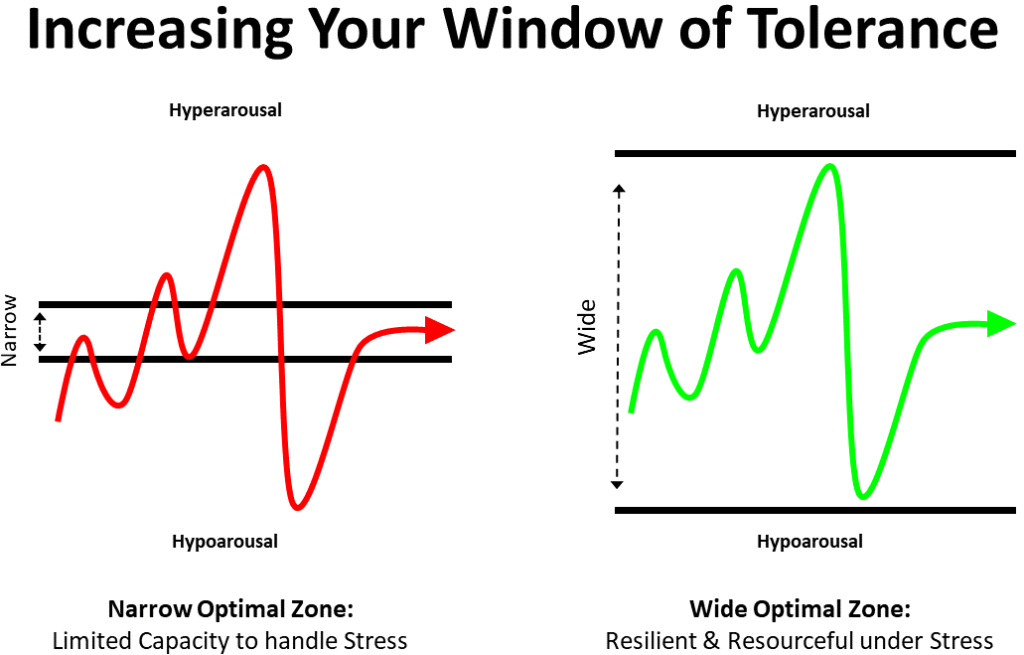
If you identify with experiencing high levels of either hyper- or hypo-arousal, this is evidence of a narrow Window of Tolerance, and once we have a better understanding of this process there are things that we can do to help ourselves.
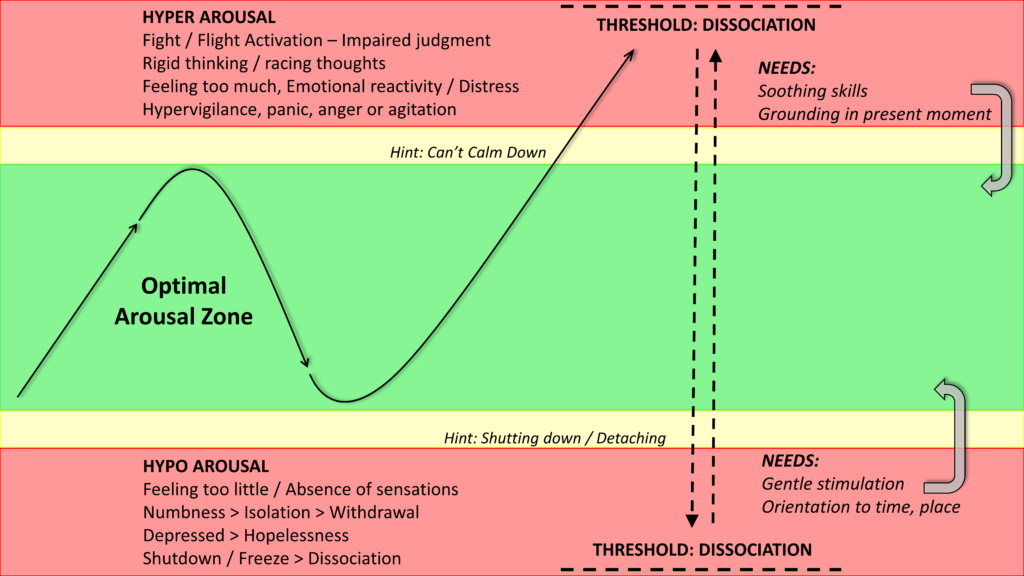
Extremes: Hyper- and Hypo-arousal (in RED):
Because Hyper- and Hypo-arousal can help to protect us from danger or distress, these states have continued to stand the test of time (i.e., through evolution, we pass on the things that ensure our survival – think ‘survival of the fittest’). However, one unfortunate common consequence of our evolutionary past is that our human brains are easily triggered by ‘false positives’. For many of us, this ‘triggering’ can happen very easily with simple imagery, painful memories and thoughts, or by focusing on threatening judgements or predictions.
This is not our fault. Rather, it is simply how our brains have evolved to protect us. We did not ‘choose’ our emotional learning histories, or to be wired the way that we are. Moreover, we are not designed perfectly. For example, although our brains have immense capacities to protect us from danger (by being able to think about and visualize all that could possibly go wrong), this comes at the cost of ‘false positives’. These are ‘bugs’ (or design flaws) and we need to learn to work with these design flaws, so that we do not get so easily triggered. This also forms part of the preparation work when building our Window of Tolerance (and you can learn more about this by reading about our brain’s Threat System, here).
Beyond the Threshold: Dissociation
Our brains have a threshold in terms of how much distress and/or arousal we can tolerate. Excessive hyper-arousal at a level that pushes us outside our window of Tolerance can lead to ‘Dissociation’, a literal disconnection or detachment from our thoughts, feelings, sensations, or memories. Equally, for some people, extreme threat can make the brain instantly ‘flip’ into shutdown, or a freeze response (i.e., extreme hypo-arousal), where we can also ‘dissociate’.
Dissociation is a huge topic, and one that deserves a separate article, but simply put: Dissociation occurs in response to extreme arousal states and/or extreme stress, as a protective mechanism to shield us from further physical, psychological, or emotional harm. Dissociation is essentially a disconnection from our conscious awareness (i.e., thoughts, memories, feelings, voluntary actions) and our sense of ‘Self’.
In essence, dissociation exists on a continuum. Although some people who experience dissociation may report that they can act in ways that they do not remember, for others, they may not even be aware that they dissociate. For instance, mild dissociative experiences are relatively common and can happen to almost anyone in response to stress or certain situations. Examples of mild forms of dissociation include daydreaming, ‘zoning out’, or getting lost in thought and ‘losing touch’ with an awareness of our immediate surroundings. This is a temporary and as will be discussed can sometimes be an adaptive response that allows our mind to take a break from overwhelming or distressing thoughts or emotions.
At a more moderate end of the continuum (as is often the case during or following an intense traumatic experience), dissociation can serve as a natural defense mechanism of the brain, that can help us tolerate what might otherwise be too difficult to bear. For some people, this may make it difficult to remember the details of a traumatic experience. In this example, dissociation is essentially a way that our brains have evolved to escape mentally from fear, pain or horror.
At the more extreme end of the dissociative continuum (as is common with people who have experienced extremely adverse events or who may have insufficiently processed trauma memories), dissociative states can literally become distinct personality configurations that are cut-off from an individual’s awareness. These personality ‘states’ or ‘parts’ may contain parts of the traumatic memory, or may represent the physical sensations, emotions or the narratives related to those events. Understandably, such shifts in consciousness may involve specific perceptions, attitudes, beliefs, and emotional responses to people and situations that are not typically held by the individual. Again, these dissociative states or ‘parts’ are not our fault. Rather, they may have emerged in response to what happened to us, and are further examples of the clever ways that our brains can evolve to protect us (i.e., to help us mentally escape from fear, pain or horror).
Often, the more extreme forms of dissociation are an indication that an individual is well outside of their Window of Tolerance. This means that no new learning can occur. This presents a significant problem for a person who is in a dissociated state whilst in a therapy session, because they may not have any recollection of information discussed. Equally, because dissociation can interfere with new learning, this can (for instance) make it very difficult to process memories in therapies such as EMDR Therapy.
Thus, if you are receiving a treatment for trauma-related memories, it is very important that your therapist understands how to assess for and work with dissociation. Dissociation is related to the Window of Tolerance because it is another indication that you first need to work on PREPARATION skills in order to do any trauma work. Invariably this phase of therapy will focus on developing skills to help you expand (and remain within) your Window of Tolerance (so you can stay in the present moment). For your own comfort, sense of safety and control, this needs to happen before you proceed to the ‘treatment phase’ of any trauma therapy. Given that dissociation is a natural response to trauma, it could be argued that is negligent of a therapist to overlook assessing for dissociation and/or failing to prepare you for the treatment phase of trauma work by doing the necessary resource-building to increase your capacity to remain well within your window of tolerance so that you can get the most out of your therapy.
How to Increase Our Window of Tolerance
It is important to emphasize that we do not get to choose how ‘wide’ the Window of Tolerance we are born with is – Different people are born with different brains and different capacities. Equally, we know that adverse events in early childhood and throughout our lives can shape our brains and can in turn affect our Window of Tolerance. Our attachment styles and early emotional learning also influence how our brains and Window of Tolerance develops.
However, although many of the negative experiences that happen to us (especially the adverse experiences we experience in early childhood) are not our fault – it is our responsibility to learn about how we can best help ourselves, because the ‘wider’ we can expand our Window of Tolerance, the more resilient we can learn to become in the face of life’s challenges.
If you would like to increase your Window of Tolerance, it will first helpful to begin to become aware of the ‘cues’ or the ‘signals’ that you are becoming either Hyper-, or Hypo- aroused. Although everyone is different, it is common for people to report that when they are becoming hyperaroused that they find it increasingly difficult to stay calm. You could use this as a signal that you are coming close to the upper edge of your Window of Tolerance and that you need to intervene.
Although different people prefer different approaches, we know that in general, calming imagery and soothing skills (such as Soothing Breathing, Safe Place or calming imagery) and grounding techniques (such as tuning into your 5 senses, mindfully) are generally what is required to bring a person out of hyperarousal back into their Optimal Zone.
On the other hand, a commonly reported signal that you may be entering hypoarousal is that you may be feeling like withdrawing or that you are ‘shutting down’. If this is the case, use this as a ‘signal’ that you are coming close to the edge of your Window of Tolerance and are moving towards the state of hypoarousal. This is a signal that you need to intervene. Grounding and containment skills are important use when outside of your Window of Tolerance.
For some people, connecting with others can be a useful way to counter their desire to withdraw. For others (particularly those with significant interpersonal traumas) connecting with others when distressed may be hugely challenging because others may be either emotionally unavailable or may be perceived as aversive or threatening. Regardless, it is helpful to have thought ahead about how you would like to respond should such a situation should it arise. In more extreme cases of hypoarousal, simple gentle but stimulating activities with a focus on grounding your experience in the present moments (i.e., techniques to help orient you to time / place) may be required.
Self-Care Strategies for Working with Hyperarousal
Working with our Parasympathetic Nervous System is hugely important when experiencing hyperarousal or are feeling are feeling overwhelmed, anxious, or disconnected. (Remember: We want to engage in soothing activities that decrease our arousal because hyperarousal is caused by an excess of Sympathetic Nervous System activity, which I discuss further here.) Therefore, any activity that involves grounding, soothing, or containment will be of benefit. Because we each respond differently to (and have differing preferences to be soothed by) different kinds of activities, it is important to develop a personal toolkit of skills and practice them regularly so that you know you can lean on them when needed. Some examples may include:
Soothing breathing (deep and slow tummy breathing, which I discuss in great detail here)
Being Mindful in nature (I have summarized the research and offered suggestions for how to do this here)
Writing things down (this can be cathartic because it can help you externalize thoughts and feelings, which can be validating and this process can help you gain perspective on what you’re experiencing; Pennebaker’s Expressive Writing Paradigm is a good example of a a structured Therapeutic Writing activity now has decades or research support and it is free. But any kind of writing that you find helpful will suffice)
Gentle stretching or Yoga (Yin / Restorative Yoga is the most soothing, but any form of working with your body in a gentle and helpful way is better than none)
Shaking, Stomping, or Vigorous Exercise (this can provide an outlet to burn off excess energy and we know the benefits of exercise continue to work for us long even after we have finished doing it)
Warm water (warm bath or shower)
Extreme cold water (when done safely, like exercise, the benefits of ice-baths are well-documented and keep working for you well after you have done this activity)
Throwing (eg, a therapy / yoga ball at a blank or outside wall, or rocks into a lake / out into the ocean)
Something rhythmical (such as dancing, rocking on a hammock, a swing, or gently bouncing on a trampoline)
Rolling on a foam roller or yoga ball (to loosen areas of muscular tension and bring you back into the present moment using your body)
Music (soothing and calming music and sounds, singing, chanting, playing an instrument)
Comforting food (eg hot chocolate or something chewy but smooth)
Lying somewhere cozy with a weighted blanket (you could combine this with soothing music, or high quality recordings of nature sounds mentioned towards the bottom of this page)
Self-Care Strategies for Working with Hypoarousal
Below are some self-care strategies to help you increase your arousal and engagement in the present moment. Any activities that involve a helpful stimulation of your body / mind, or that may include grounding you in the present moment safely are likely to be useful here. Remember, because we each respond differently to different kinds of activities (and have differing preferences for stimulation), it is important to develop a personal toolkit of useful actions that you enjoy and to practice using these skills regularly so that you know that you can lean on them when you most need them. Essentially, anything that stimulates the prefrontal cortex and/or brings you into the present moment safely is what we are looking for here. Some examples may include:
Sensory Stimulation (anything that you can do Mindfully while engaging your 5 Senses could be helpful; Anything that stimulates the prefrontal cortex and/or brings you into the present moment safely is what we are looking for)
Movement / Vigorous exercise (choose something intense, simulating or that challenges your co-ordination in someway, for instance a hand – or head – stand against a wall, or try walking backwards for 3 mins on your hands and feet with your belly facing upwards)
Body Scan: Start by focusing your attention on your toes and gradually move upward, paying attention to each part of your body. Notice any sensations, tension, or relaxation in each area. (This exercise helps you connect with your physical sensations and brings you into the present moment.)
Balancing or Dancing (or any physical activity that increases your heart rate and gets your body moving; something that is challenging will also bring you into the present moment because it demands your attention)
Smelling essential oils (smell is the fastest way to the thinking brain)
Chewy crunchy food (the sounds and sensations can be a source of stimulation)
Jumping on a trampoline or mini trampoline
Finger painting, drawing or art (provides and opportunity for tactile stimulation, and present-moment decision-making and problem-solving)
Listening to Stimulating Music (or playing an instrument)
Water play with a straw (blowing through the straw)
Cold water Immersion (the invigorating positive effects of cold water and ice baths are now well-known)
Holding a piece of ice until it melts (this can be quite challenging and aims to help you return to the present moment)
Increasing your cognitive load (eg Look left, name 3 things, and list 3 facts – not judgments, but facts – about those things. Then look right and do the same. You could repeat this and aim to find 3 new things each time.)
Alternatively, you could make use of “5-4-3-2-1” (Name five things you can see, four things you can touch, three things you can hear, two things you can smell, and one thing you can taste. This exercise engages your senses and helps redirect your attention to your immediate environment.)
Contact a friend and focus on meaningful connection (even though this may be the opposite of what our nervous system is pulling us to do)
For certain people, such as those with a narrow Window of Tolerance (which is understandably common in people who have experienced significant traumas or stress), there can be almost zero warning that they are entering either Hyper- or Hypo-arousal. This is not their fault. Rather, it is the result of the trauma, and how trauma affects our brains – it makes the brain over-protective to prevent any further harm.
However, unfortunately, this can sometimes take people by surprise and they can lash out at others (‘attack’) or themselves, or can completely shut-down (‘withdraw’), and this may leave a person feeling ashamed, or powerless and out of control of their emotions. If this is the case (if this is you, or someone that you care about), please understand that self-help techniques alone will likely only be of limited use. When this is the case, consulting with an experienced, trauma-informed clinical psychologist is highly recommended.
If you are receiving Therapy – especially EMDR Therapy – and you are working with trauma or painful memories, it is your Therapists’ upmost ethical and professional responsibility to determine what your Window of Tolerance is, and to work safely with you to help teach you what you do not know so that you can develop the skills that you missed learning. That way, the work that you do together will be as efficient and effective as it can be.
Summary:
“Window of Tolerance” is a term used to describe the zone of arousal in which a person is able to function most effectively.
When in the optimal zone, we are calm but alert and we can be engaged in what we are doing.
When we are outside our Window of Tolerance, either we are in Hyper- or Hypo- arousal and we need to take specific steps to bring ourselves back into the Optimal Zone.
Much like how the thermostat in an air-conditioner makes micro-adjustments to temperature to keep it within a comfortable range, staying within the optimal range of our Window of Tolerance requires the awareness and skills to attend to our needs and to regulate out arousal level to match the situation at hand
We can do this either with self-soothing when we need to Deactivate our arousal, or via activities that stimulate us when we need to Activate our arousal
The size of our ‘window’ depends upon how much we are able to tolerate fluctuations in mood, energy levels, and the challenges and demands of life, whilst remaining in the Optimal Zone.
We do not get to choose how ‘wide’ the Window of Tolerance we are born with is – different people are born with different brains and different capacities.
Adverse events in early childhood and throughout our lives can shape our brains and can in turn affect our Window of Tolerance.
Although many of the negative experiences that happen to us (especially the adverse experiences we experience in early childhood) are not our fault – it is our responsibility to learn about how we can best help ourselves, because the ‘wider’ we can make our Window of Tolerance, the more resilient we can learn to become in the face of life’s challenges.
We can increase our Window of Tolerance by practicing mindfulness, building social connections, improving lifestyle factors known to reduce stress (e.g. healthy nutrition, regular exercise, and getting adequately restful sleep) and by seeking out mental health support
If you are in Therapy – especially EMDR Therapy – and you are working with traumatic memories, it is your Therapists’ upmost ethical and professional responsibility to determine what your Window of Tolerance is, and to work safely with you to help teach you what you do not know so that you can develop the skills that you missed learning.
I am a PhD Clinical Psychologist and EMDR Accredited Practitioner with over 15 years of psychotherapy experience. Whether you are seeking an assessment and diagnosis, or are searching for integrative research-backed ways to help you heal past wounds, break reactive-patterns and achieve long-lasting change, my aim is to provide a safe space for you to feel seen, understood, and empowered so you can make meaningful progress on your healing journey.
I endeavor to reply to all enquiries within 24 hrs.
About Me:
Dr Andreas Comninos, PhD Clinical Psychologist
I am a PhD Clinical Psychologist and EMDR Accredited Practitioner with over 15 years of psychotherapy experience. Whether you are seeking an assessment and diagnosis, or are searching for integrative research-backed ways to help you heal past wounds, break reactive-patterns and achieve long-lasting change, my aim is to provide a safe space for you to feel seen, understood, and empowered so you can make meaningful progress on your healing journey.
EMDR Therapy is a distinctive and efficient method for addressing painful memories and negative beliefs, initially developed over 30 years ago to treat post-traumatic stress disorder (PTSD) resulting from significant traumatic events.
We know from extensive international research spanning decades that EMDR Therapy’s effectiveness extends far beyond addressing life-threatening traumas – It can heal developmental wounds that underlie a wide-range of psychological and behavioural problems.
EMDR Therapy essentially rewires your brain to heal wounds from past events, alleviating ongoing disturbances, and reducing negative self-perceptions and habitual reactions to new situations.
Fast Facts:
EMDR Therapy was developed over 30 years ago by psychologist Francine Shapiro, and is now backed by decades of research.
In 2013, EMDR Therapy was recognized by the World Health Organization as a first-choice treatment for trauma.
In 2018, the Australian Psychological Society included EMDR therapy as a Level I evidence-based psychological intervention for posttraumatic stress disorder in adults.
In 2020 EMDR Therapy was included by Australia’s Medicare Better Access Scheme as being the only one of two other therapies deemed an ‘acceptable strategy’. This important because it is the first time any therapy has ever been added to this list by Medicare (in the entire 10+ years history of the Better Access Scheme).
Recovering From Our Past
In practice, ‘trauma’ is not about the event itself. It is about what happens inside us in response to an event. A traumatic response is essentially an unfinished set of reactions to something. In other words, this is any haunting or destructive material that is left inside us (emotionally, in our minds and / or in our bodies) following a disturbing event. This can be caused by any event that we experience as emotionally distressing – not just life-threatening events.
While the formal diagnostic criteria for Post-Traumatic Stress Disorder (PTSD) lists large, obvious, single-incident events that are typically life-threatening, this is actually misleading because many people are also affected by other adversities that do not meet any formal diagnostic criteria. These experiences commonly include interpersonal injuries such as: Betrayal, the loss of a significant relationship, Attachment wounds, Emotional Abuse (gas lighting, bullying or harassment), and any other experience that can result in extreme humiliation/shame, fear, or a loss of control or feelings of insignificance.
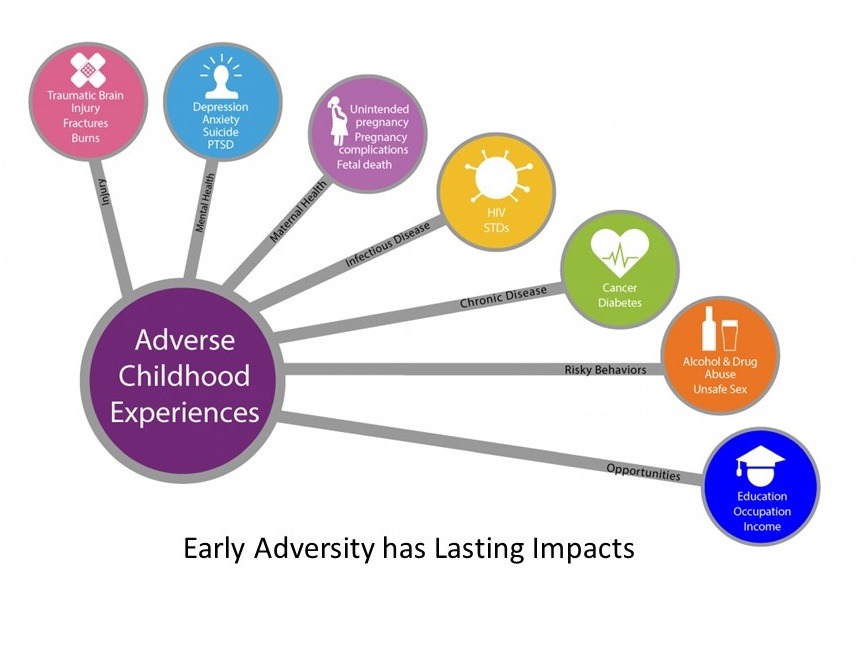
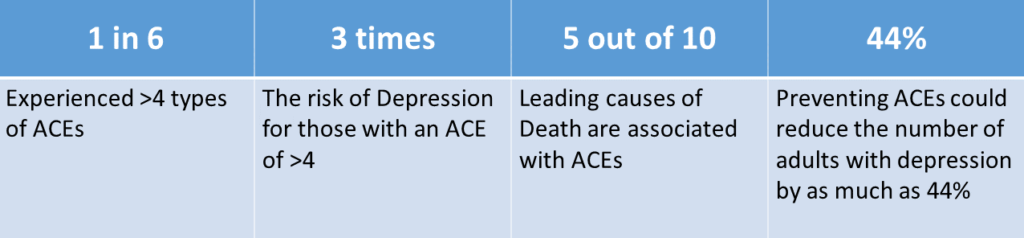
Left untreated, adverse events experienced as traumatic can leave a huge and long-lasting negative impact on our mind, body and emotions that can leave us vulnerable to present-day stress and future triggers. Moreover, the effects of untreated trauma can also be passed on inter-generationally. In addition to the emotional and physical effects, the long-term cumulative effects of unresolved traumas can trigger a complex reorganization of the brain and body that can make us more prone to serious mental health and medical/physical complications.
In children, we now know that the cumulative effects of unresolved adverse childhood experiences and painful attachment experiences can have a negative impact on general brain development. This can affect a child’s emotional and cognitive development and can negatively impact on resilience (i.e., our ability to handle stress, to regulate our emotions, and to bounce back from significant setbacks).
We now know that the risk of developing mental and physical health problems increases with the number of untreated adverse events we experience. This is because the accumulation of painful experiences over time can have a significant, long-lasting negative impact on how our brains develop and function (particularly if these events repeatedly happened during childhood). This has far-reaching implications for how we store and recall existing information, and how we interpret and respond to new information, which ultimately affects how we act and feel about ourselves (and others).
This partly explains why two adults who may experience the same traumatic event may handle it very differently. One person may ‘bounce back’ and ultimately be unaffected in the longer-term, whereas for the other person (if they have vulnerabilities due to having a history of many similar unresolved traumas), the event may be experienced as debilitating and may either ‘confirm’ beliefs they hold about their world which may continue to affect them for years to come. Thankfully (as will be discussed) with EMDR Therapy it need not be this way.
Resolve the Memory, Resolve the Problem
The theory underpinning EMDR Therapy views the majority of emotional, psychological, and behavioural problems as being related to ‘stuck’ (unprocessed) memories. It follows that by identifying and reprocessing these memories safely, a person’s emotional, psychological and behavioural diffisulties will also resolve. This is exactly what we observe following EMDR Therapy. Here is a brief summary of key points about this therapy:
Over the past 30 years, EMDR Therapy has been extensively researched and validated as a very effective approach for BOTH single-incident (life-threatening) and also repeated (non-life-threatening) interpersonal traumatic experiences.
There is also strong research support that EMDR Therapy is useful for a wide range of behavioural and psychological difficulties including: Depressive disorders, all forms of Anxiety (Panic, Phobias, Social Anxiety, PTSD, OCD etc), Addictive and Compulsive behaviours, Eating Disorders, Chronic Pain, and Complex Trauma (c-PTSD).
EMDR Therapy is also useful to for non-diagnostic difficulties, such as attachment-related wounds, intense shame and self-criticism (which is often related to having a painful attachment history).
There is also emerging research demonstrating that EMDR Therapy is effective with helping people manage Chronic Pain and also medically-unexplainable physical sensations (also known as ‘somatoform disorders’).
Benefits: Results without ‘talking’
Although we cannot erase a memory, we now know from over 30 years of research that memory processing done via EMDR Therapy results in a complete elimination of the disturbance associated with the memory. Moreover, we know that with this change, comes positive associations (positive, adaptive self-beliefs). In addition, these changes become the new normal – a new foundation that all new learning and subsequent experiences are encoded.
Unlike most talking therapies, the processing of memories via EMDR Therapy involves very little talking. Early on, the therapy involves taking a history, and also determining yourwindow of tolerance (for your safety).
Preparation for memory processing involves teaching you the skills you need to stay within your window of tolerance (this may take several sessions depending on your needs). Following this, you will be well resourced for the memory processing phase of treatment (which often can happen very quickly – in as little as a single session).
Your therapist will then develop with you an EMDR Treatment Plan, which identifies patterns and orders your past experiences related to different themes in terms of Past Events (Memories related to that theme), Present Triggers (i.e., “Every Time ‘X’ happens, I still get triggered”), and Future Templates (What you ultimately would like to achieve as a result of processing memories within that Theme – how you would like to be able to respond to the Present Triggers). This process will help you and your therapist identify which experiences most significantly relate to the Theme in question, and which memories you will likely need to Target.
With EMDR Therapy, you get to decide which Theme you would like to work on and which memories you would like to Target and resolve. You may choose to start to work on processing the earliest memories, the most disturbing memories, or a recent memory / trigger.
Memory processing involves recalling certain features of the target experience and noticing with your therapist: what you feel in your body, what emotions you may be experiencing, and any beliefs about yourself that you may have. This happens in the presence of 10-20 seconds of bi-lateral stimulation provided by your therapist (which most commonly takes the form of eye-movements, but it can also include tapping, or auditory bi-lateral stimulation).
Overall, there is very little talking that occurs. Your therapist will periodically check in with you to ensure that you are on track to resolve the memory (taking cues from the things that you report that you are ‘noticing’ after each set of bi-lateral stimulation).
We know that the processing of a memory is complete when bringing up the original image actually no longer disturbs you. Instead, you will feel calm and will have new positive associations / beliefs about yourself. People are often very surprised to find that this can happen in as little as 1-2 sessions, even for very old and painful memories
How EMDR Therapy Works:
Freeing ‘Stuck’ Memory Networks
When we experience a painful event, it can often become ‘stuck’ in our mind in the form of a painful unprocessed memory (which may have imagery, sounds, smells, emotions, bodily sensations and/or beliefs associated with it). Depending on the severity of the painful event, these memories may not resolve on their own. This can create ‘fragments’.
We know this has happened whenever the memory of an event still causes us disturbance, or when we are triggered by similarities in present-day experiences that in someway relate to a previous event – even if it happened years before and we may not often think about that link consciously. Healing past pain and removing any ongoing vulnerability is precisely what EMDR Therapy can us to resolve.
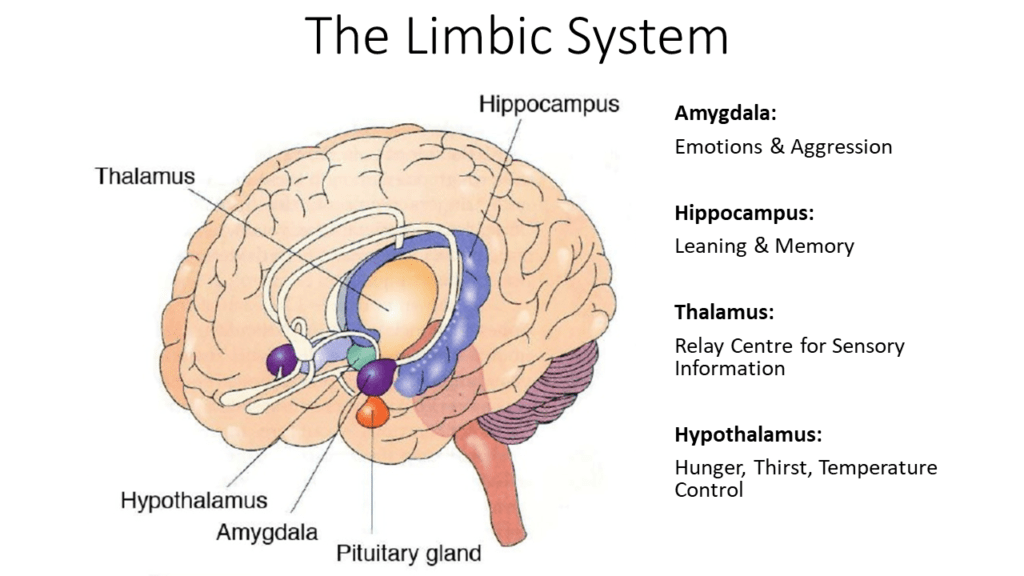
How?Normally, events from each day are processed by our hippocampus (short-term memory storage) and integrated into to our cortex (where longer-term links are made) during sleep. However, the content from disturbing memories is ‘stuck’ and becomes held in a raw or unprocessed state in the limbic system (which is essentially our Threat System). This keeps the distressing elements of the memories ‘alive’. When a new experience triggers any of the related elements of the memory, the event may feel like it is happening again, NOW. This can become very debilitating.
During a memory-processing session (which does not happen without a thorough assessment and skills building, which may take several sessions), you asked to recall specific components of the problem memory as directed by your therapist – this may include its image, the negative self-belief, and/or the disturbing emotions and associated body sensations. This will happen while simultaneously engaging in bilateral stimulation (i.e., stimulation involving both sides of the body) such as left-to-right eye movements (self-administered ‘tapping’, sounds alternating between each ear, or flashing lights). Eye movements are the most common bilateral stimulation used and these are believed to mimic the eye movements of REM sleep (the stage of sleep responsible for memory processing and learning). These eye-movements may be repeated quickly, in sets of 20-30 (several times), until processing has completed.
In this way, the EMDR Therapist systematically treats each of the stuck components of an unprocessed memory (described above) using bilateral stimulation to help your brain store this information in new ways. In doing so, the information that was once held in a ‘stuck’ memory network is reconnected to more functional memory networks, where a person can make better sense of what has happened. This leaves a person feeling resolved (vs ‘stuck’) about the corresponding memory and its components.
A Simple Metaphor: Disk Defragmentation
A simple analogy is that our brains can become a lot like a mechanical computer Hard Disk requiring a regular disk defragmentation to perform optimally. Without a regular disk defragmentation, a Hard Disk can become slower and can experience processing errors due to the information it holds becoming ‘fragmented’.
Inadequately stored (or incomplete processing of) past information can create dysfunction in our Brain’s Memory Networks and this results in inefficiencies in how our brains process and store new information (leading us to become ‘triggered’). EMDR Therapy is like performing a Disk Defragmentation on our Brains, for past experiences that did not get fully metabolized. EMDR Therapy helps our brains de-fragment, integrate, and store the past in a more helpful and efficient way.
Although we cannot get rid of a memory, it is possible with EMDR Therapy to remove the distress and disturbance that was once associated with this memory. We know that processing is complete because we find that the original memory no longer causes any disturbance. In other words, after processing a memory using EMDR Therapy, bringing up this memory or any of its components will still be possible, but doing so will no longer bother you anymore (processed memories become resolved). For example, a painful experience may still be ‘awful’ or ‘sad’, but after EMDR Therapy, bringing up the memory that you have about this event will no longer cause you any disturbance. Instead, you will feel calm and will have new positive associations / beliefs about yourself.
Returning to our analogy of a computer– Like defragmenting a Hard Drive helps a computer run better, EMDR Therapy helps the brain to metabolise previously ‘stuck’ memory networks (which can contain previously intrusive Imagery, Sensations, Emotions and Self-beliefs) so that it can operate more efficiently. Like defragmentation, this information is not ‘erased’. Rather it is reorganised to become (and is transformed into) adaptive material where you can recall the past, but it doesn’t affect you anymore and healing, letting go, and/or positive changes can occur.
In other words, when a previously dysfunctional ‘memory network’ has been processed with EMDR Therapy, the information becomes ‘adaptive’. When this happens, many positive changes occur alongside this process: Emotions associated with the past event become ‘clean’ vs the ways they used to seem disproportionate (eg instead of fear, you will feel safe and calm; you will be able to experience appropriate sadness without this emotion overwhelming you or it feeling ‘unsafe’; when thinking about a failure or a setback you will be able to feel ‘clean disappointment’ without the setback ‘saying something’ negative about your deeper worth as a human being; or, instead of anger feeling consuming or toxic, you may still feel anger if it is justified but will feel an appropriate amount of emotion where you are not overwhelmed and can choose your next response without reactivity). People are often very surprised to find that even when a particular memory is very old and/or painful, that this change can happen in as little as 1-2 sessions.
Before EMDR Therapy:
When we experience an intense adverse experience that is too overwhelming for our Brains to make sense of, this information forms a ‘stuck’ or dysfunctional Memory Network (with associated feelings, sensations, sounds, smells, and beliefs about ourselves).
Experiences that are ‘stuck’ have not been fully processed – they carry an emotional ‘sting’ or can cause us pain when we remember them.
Because we draw on our Memory Networks to make sense of the world, we remain forever vulnerable to being triggered by any present events where there is enough similarity.
This may cause us disturbance, may pull us into the past, or may leave us open to being reactive.
Dysfunctional Memory Networks often relate to one or more negative self-referencing beliefs (eg ‘I am bad’ / ‘I’m unlovable’ / ‘I am in danger’ / ‘It’s my fault’ – and other self-referencing negative cognitions that typically cluster around themes of Guilt, Shame, Vulnerability, Control, or Belonging).
After EMDR Therapy:
We are free to choose to recall a painful event and doing so does not disturb us.
We feel resolved about a previously negative situation (‘it happened, it is in the past, I am SAFE now’), and the memory of it does not affect our view of ourselves.
Things that used to trigger us no longer do – we become free to choose how we want to respond
We can connect with a more positive view of Self (eg ‘I am loveable’ / ‘I did the best that I could’ / ‘I am safe now it is over’ and other positive self-referencing cognitions).
We are free to have new experiences which strengthen the memory processing done in EMDR.
This then becomes an adaptive lens through which all new events are viewed.
Before and after EMDR Therapy
EMDR Therapy & Sleep
Bi-lateral stimulation is unique aspect of EMDR Therapy. This is believed to relate to how the brain processes memories while we are a sleep. One of the most important stages of sleep in terms of learning and memory is called ‘rapid eye movement’ (REM) Sleep. REM sleep is where we consolidate learning and memories from the previous day. A key component of REM sleep is bi-lateral eye movements (our eyes flicker left-to-right). You may have seen someone’s eyes doing this when they are sleeping – chances are that they were in REM sleep and were processing memories.
Therefore, EMDR Therapy makes use of this process by mimicking the eye-movements of REM sleep to stimulate the brain’s natural way of storing memories. This can be done by using bi-lateral stimulation (i.e., using both sides of the body) such as left-to-right eye movements (or sounds, flashing lights, or ‘tapping’).
Interestingly, regarding sleep – we know that people who do not sleep well do not learn well. For example, studies investigating the benefit of sleep for learning a new task have found that people who learn a complex task before bedtime do better in the morning than participants who were taught the same task in the morning but were tested in the afternoon. Studies deliberately interfering with REM sleep (using alcohol – a substance known to interfere with REM sleep) have also demonstrated that a disturbance to REM sleep directly affects memory consolidation and learning.
Clearly, sleep is important for learning and memory. We know that people do not experience good quality sleep when they are distressed. Distressing dreams are common to people who have experienced significant stress or trauma. We also know that REM sleep is important for storing memories and processing emotions. When REM sleep is disturbed, emotional distress may accumulate. People who have experienced trauma or significant emotional distress often report that they are haunted by persistent and intrusive imagery, thoughts, and memories (e.g., rumination, intrusive thoughts, and flashbacks). As previously discussed, many of these are in fact components of unprocessed memories. This indicates a relationship between unprocessed memories and poor REM sleep.
Again, EMDR Therapy identifies a stuck memory (and its components) and carefully stimulates this information, while pairing it with the bilateral eye movements observed in REM sleep. This in turn allows the brain to process the memory. By mimicking the eye-movements of REM sleep, or by using other forms of bi-lateral stimulation (i.e., using both sides of the body) such as sounds, flashing lights, or ‘tapping’, EMDR Therapy facilitates the brain’s natural way of processing a memory that was previously ‘stuck’. This results in an elimination of distress associated with the memory – and with this, comes a resolution of the related emotional, psychological and behavioural problems people were originally experiencing!
Getting past your past: What’s the Catch ?
Less Talking…
EMDR Therapy is very different to all other talking therapies. During the memory-processing phase, talking is kept to a minimum. In fact, while a memory is being processed using the bi-lateral stimulation (e.g., left-to-right eye-movements) very little talking occurs at all (!).
The only talking that does occur is simply for the sake of a brief check-in, so that the therapist can check in with you to ensure that you are still processing the memory.
For example:
Therapist: “OK – take a breath. What do you notice?”
Client:“I feel something in my chest and shoulders”
Therapist: “Ok – Notice that…” (Bi-lateral stimulation continues until memory is processed…)
Notice that in the above example, unlike typical ‘talk’ therapies, in EMDR Therapy the therapist does not ask the client about what their sensation might relate to, what their sensation ‘might’ mean, or why they think they are experiencing their sensation.
Instead, there therapist is simply checking to make sure that memory processing is still occurring.
This is very different to regular talking therapy.
Worse Before Better
Sometimes during the processing of a painful memory, your distress may increase. This is normal – and it is OK if you have the skills to calm, ground, and soothe yourself, so that processing can continue. Without calming, grounding and soothing skills, processing a painful memory could become very difficult. If you have not done this necessary preparation work with your therapist, you may find this very emotionally challenging.
Often, therapists who are overly eager to get to processing memories with their clients may rush through this preparation stage. However, processing a memory without adequate preparation is insensitive to you and your needs, and this could become unsafe for you – it could even make things worse.
Although this preparation work may take several sessions, it is important to do this thoroughly. Preparation will typically involve exploring your Window of Tolerance and your triggers, and teaching you numerous ways to calm, ground and soothe yourself (for example, by using soothing breathing, mindfulness, and calming imagery). These skills are also helpful to use in-between therapy sessions – even if you are not yet at the memory processing stage of EMDR Therapy.
Without this preparation work – I do not recommend processing memories via EMDR Therapy. If you are reading this and your therapist has not prepared you for memory processing, please give them the following article to read: Understanding your Window of Tolerance.
It Can Work Fast, but….
Processing a memory can happen very quickly. Often, a previously disturbing painful memory can be reprocessed and relieved, within 1-2 sessions (!). Although this may sound impossible, it is actually quite commonplace (remember, EMDR Therapy is supported by over 30 years of research). However, there are some important considerations to be aware of:
For more complex issues, there may be a network of multiple thematically-related memories that need to be processed before a full relief from disturbance is achieved. This is often the case with complex trauma (for instance).
Essentially, preparation for memory processing involves numerous steps: Taking a History, mapping out how your memories cluster into themes, determining your Present Triggers and Future Goals, establishing your Window of Tolerance (see the image below), and building skills so that you can handle any difficult emotions that may show up as when you bring up the memories that are affecting you.
Although EMDR Therapy can produce results very quickly, some people require several preparation sessions before they are ready to process memories. In essence, this preparation phase is focused on helping you to manage your symptoms skillfully, to a level where you are able to tolerate bringing up the memories that are affecting you. These skills will ensure reprocessing past memories with EMDR Therapy is comfortable and safe.After all, the last thing anyone wants is to create further negative associations with painful memories. Some people may need time to work on these skills.
EMDR Therapy is often wrongly referred to as ‘EMDR’ (which connotes it is a ‘technique’). In other words, people often falsely assume that ‘EMDR is just the eye movements’. However, ‘EMDR Therapy’ is a comprehensive approach to helping alleviate human suffering that encompasses many elements of other therapies (the depth of which is determined by the skills / experience that the therapist brings).
Although the ‘eye movements’ are commonly mistaken as the ‘EMDR’ part of the therapy, in actual fact there are 3 distinct Stages of EMDR Therapy. As you will see, these Stages make it a highly nuanced and comprehensive Therapy (vs ‘just a technique’).
Assessment Stage
Preparation Stage
Treatment Stage
Assessment Stage: Assessment is common to ALL therapies. The assessment Stage includes taking a detailed history, trying to understand your goals for seeking treatment (i.e., including understanding why you happen to be seeking help now at this point in your life specifically?), identifying the maintaining factors (that keep your problem continuing), identifying your skill set and any relevant risk factors, identifying potential clashes in the therapeutic relationship or challenges in terms of your expectations regarding what can be achieved in therapy (vs the work / effort you’re willing to invest), and trying to arrive at a conceptualization that helps explain how past events relate to the present difficulties you may be having so as to determine what will be most helpful. (You can read more about what to expect in therapy and how to get the most out of these early sessions here.)
If the Assessment Stage is skipped and you jump straight to any treatment, important information may be missed and this could mean that you are not given the most appropriate treatment for your issues or goals.
Although the Assessment Stage is presented above as a distinct entity, in practice a good Clinical Psychologist is ostensibly always in ‘assessment mode’. They may be monitoring your understanding, assessing how a skill or treatment is fitting with you, assessing for any signs that indicate a change in your Window of Tolerance, or determining the approach being taken is ultimately what you need. In other words, there are often several reasons behind why a Clinical Psychologist asks you the questions they do and makes the recommendations that they make – and if you are curious you should ask what their reasoning is and they should be able to tell you.
PreparationStage: This Stage of therapy involves teaching you skills that will make doing the work of therapy (the Treatment Stage) SAFE for you. This Stage shares overlaps with the Assessment Stage and may include: determining your physiological Window of Tolerance, your capacity to self-soothe / self-regulate, determining what activities you needs and which you respond best to (and you prefer). This stage can incorporate skills from ANY therapy – anything that is helpful is useful at this stage (eg, ACT, CFT, IFS – any therapy that can be tailored to your unique situations / needs). The duration of this stage of therapy is informed by information from your assessment, and also from your response to these activities. Sometimes people may need to spend several months working at Preparation. A related area in Preparation is the development of an EMDR Treatment Planner – which is essentially a live document designed in collaboration with you that organizes into Themes your TRIGGERS (and the underlying historical experiences that likely feed into those triggers) and your GOALS.
Because EMDR Therapy is very specific and probably unlike anything you have ever experienced before, it is common for therapists to take you through an example of what happens in an EMDR Therapy session using a recent trigger you have experienced that is only moderately difficult. That way, you will be able ‘see’ what a typical re-processing sessions of EMDR Therapy entails. By picking something ‘easy’ to do this with, you will be able to have your attention ‘in’ the experience of re-processing, while also able to ask questions about what is happening. It is kind of like playing an ‘open-handed card game’ until you understand what is required to get the most out of EMDR Therapy. Only then will you be well-informed and ready to apply EMDR Therapy to more significant and challenging material.
If the Preparation Stage is skipped, negative outcomes can occur. You may find the work highly triggering or you may not have adequate skills to settle and soothe yourself in-between sessions.
Poorly trained therapists often skip or rush the Preparation Stage to get to the Treatment Stage. This does a MASSIVE disservice to the public who may then be at risk of being triggered by EMDR Therapy and who may otherwise discontinue receiving a treatment from which they could have greatly benefited. Sadly, I have met many individuals who have had negative experiences with previous therapists, who needed my help to heal from prior therapy.
Treatment Stage. This is where EMDR Therapy differs THE MOST from other therapies, because the amount of ‘talking’ that happens in most other therapies stops in EMDR Therapy. As is discussed in the remainder of this article – the application of bi-lateral stimulation to each of the specific components of unprocessed emotional experiences (the image, the negative view of your Self, the emotion/s and your somatic experience), is what makes EMDR Therapy very different to other therapies.
A common misconception is that because EMDR Therapy uses eye-movements, it is “a form of ‘hypnosis’”. This is completely inaccurate – Although hypnosis may use eye-movements (or other forms of stimulation / sounds), hypnosis uses the ‘power of suggestion’ in the hope that you feel different. ON the other hand, EMDR Therapy works with how past experiences are represented in your mind, body, and emotional experience, and it helps your brain re-process this material so that it can be stored in more helpful ways. There is no ‘power of suggestion’, rather, your brain ‘re-processes’ the past and then files away this information where it belongs – in the past (in your long term memory), and as a result you are no longer triggered in the present. You can read more about the differences between hypnosis and EMDR Therapy in the ‘MYTHS & MISCONCEPTIONS’ section at this bottom of this page).
Imagery Rescripting & EMDR Therapy
Once you feel comfortable with reprocessing an experience with EMDR Therapy, more advanced options are available. One of these involves combining Imagery Rescripting within the framework of EMDR Therapy. Imagery Rescripting is an evidenced-based way to help people creatively resolve either upsetting memories, nightmares, and/or upsetting imaginings of the future.
Rescripting may involve considering how you would like the image to be different, what you would like to do to the image to make it less threatening or for you to feel safer, or what you are needing in the image and finding ways to rewrite the story to meet that need.
A common misconception becomes obvious when clients say ‘but I can’t change the past’. YES – This is 100% correct: We cannot change the past and that is not our aim. Rather, with imagery Rescripting we are working with the way your brain has stored / is representing the past. Imagery Rescripting in conjunction with EMDR Therapy is particularly helpful for healing attachment wounds and resolving other adverse experiences from early childhood. This can also be helpful for future events.
However, combining EMDR Therapy with Imagery Rescripting requires that the Assessment and Preparation Stages to have been completed. It is also helpful to be well-resourced in self-regulation and grounding skills and to be familiar with the standard way of doing EMDR Therapy if you are interested in adding this additional deeply healing component.
EMDR Therapy Animations:
The following brief animations explain how EMDR Therapy works. As you watch, remember that although EMDR Therapy was originally developed for large and obvious single-incident traumas, it has since been found to be highly effective for healing from all sorts of Adverse Events that can otherwise continue cause us psychological, emotional, or physical harm. This is because that when left untreated, the pains from our past combine and accumulate, resulting in ongoing vulnerabilities for us to be triggered by the present. Unless we resolve the past, we will continue to be affected by it past indefinitely and this is what can often fuel psychological and behavioural problems ranging from from anxieties, relationship issues, low moods, and addictions.
Thankfully it need not be this way. Although we cannot erase the past, by safely re-processing the pains of the past using EMDR Therapy, we can heal our brains, and the past will no longer affect us the way it once did. By using bi-lateral stimulation (vs talking), EMDR Therapists work with how your brain represents the past to achieve a resolution safely and quickly (with very little need to talk about what happened).
An animation explaining EMDR Therapy:
An animation from UK’s EMDR Association:
Common Questions:
Do I have to process every memory I’ve ever experienced ?
Thankfully NO, because this would take a long time. Due to what is known as the ‘Generalization Effect’, often processing an event or memory may also help reduce the disturbance you experience in response to similar memories.
The Generalization Effect works in the following way – imagine you were going to cut back a huge, thorny rose bush: You could start at the most recent flower and trim the bush backwards to the most recent leaf, then work backwards to the nearest branch (etc…). Alternatively, you could start much lower down, and with one or two ‘snips’ you could remove large sections of the bush because everything stems from the earlier, more established branches. On the other hand, if you wanted to remove the entire bush, you could do so by going directly to the oldest part of the bush (the trunk). However, the thorns from the branches may make that difficult, so (luckily) you have the above options.
Because of the Generalization Effect, processing memories with EMDR Therapy is similar to the above Rose bush metaphor – you could start at the most recent memory, the earliest memory, or the most painful memory. There are pros / cons to each. However, most of the time, resolving an earlier memory has the biggest flow on effect for all subsequent memories. It is like trimming the rose bush low down at its trunk (all other branches will thus be affected).
Determining where to start is up to you. However, before memory processing can begin, an important phase of treatment involves working with your therapist to formulate a Treatment Plan. This is often written up into a table, which clusters the memories that disturb you and bought you to EMDR Therapy, into ‘Themes’.
The EMDR Treatment Plan orders your experiences related to each Theme in terms of Past Events (Memories related to that theme), Present Triggers (i.e., “Every Time ‘X’ happens, I get triggered”), and Future Templates (What you ultimately would like to achieve as a result of processing memories within that Theme – how you would like to be able to respond to the Present Triggers). This process will help you and your therapist identify which experiences most significantly relate to the Theme in question, and which memories you will likely need to Target.
With EMDR Therapy, you get to decide which Theme you would like to work on and which memories you would like to Target. You may choose to start to work on processing the earliest memory, the most disturbing memory, or a recent memory / trigger. Your therapist can assist you to learn skills to help support you through the memory processing safely, so that you can remain within your Window of Tolerance whilst processing a memory / experience.
Thanks to the Generalisation Effect, you do not need to process every experience or memory related to that theme that you have ever had.
What if I Can’t Remember the Past?
There are many reasons why we have ‘foggy’, incomplete, or even very little recollection of the past. Sometimes people ‘know’ that an event happened, but they cannot remember the experience. Other times, people report that there is no specific event that they can remember, because the same painful experience happened over, and over again (or happened many times throughout long periods of their development).
However, with EMDR Therapy, it is not necessarily important that you remember the ‘facts’ of an event.
Why? Because EMDR Therapy works on how a memory is encoded (stored). The ‘facts’ are not necessarily what is most important. Rather, how your brain ‘represents’ the past is what we are working with in EMDR Therapy.
Sometimes, you can literally create a scene in your mind that captures an event or a period of your life, and your therapist can work with you and that scene to extract the significant material that captures what has been left by that experience. This is because just as a memory has specific components, a scene that you have created in your mind will also have these components. Any of the components in that scene can be used as a Target for memory processing.
Again, EMDR Therapy is working with what has been left in your brain by the past (i.e., how the past is being represented in your mind). This frees you up from having to remember ‘everything’ from your past.
Is EMDR the Same as Hypnosis?
No – In hypnosis, you are guided by a therapist to enter an altered, trance-like ‘hypnotic state’, which is thought to bypass the conscious, analytical mind. This is thought to make a person more open to accepting positive suggestions. Therefore, in Hypnosis, you are encouraged to act or feel differently by the therapist’s ‘use of positive suggestion’ about a pre-determined goal or behaviour.
In contrast, the tasks of EMDR Therapy are driven by what we know about how memories are perceived, stored and retrieved. In an EMDR session, a person does not go into a trance-like state of consciousness, because this would actually be counter-productive to processing a memory. This is why steps are taken by the EMDR Therapist to pre-determine your Window of Tolerance (because memory processing cannot happen if you are not mentally ‘present’).
Therefore, in EMDR, active attempts are made towards repeatedly grounding a person in the present moment, by asking them to remain highly focused on specific things (like eye-movements, physical tapping or other forms of bilateral stimulation), while checking-in with their current feelings and body sensations. In EMDR, the therapist is deliberately doing this to prevent you from drifting away from reality, because memories cannot be processed if you are not consciously present.
In EMDR Therapy, we are working with your memories until you have processed them, and you remain in control at all times.
Will EMDR Erase Memories?
No – EMDR Therapy cannot not get rid of a memory. EMDR Therapy also cannot change that fact that past negative experiences happened to you. That is not the goal. You will still have the memory, but it will not disturb or bother you any longer.
EMDR Therapy will change (for the better) how you feel when you bring a past event or memory to mind. EMDR Therapy specifically targets the components of stuck memories, so that they are moved from your limbic system to your pre-frontal cortex where a person can make better sense of what happened. This then allows adaptive learning and new (positive) information to be integrated. This leaves a person feeling resolved (vs ‘stuck’) about the corresponding memory and its components.
In other words, after processing a memory with EMDR Therapy, you will still have access to the memory, but it will not cause you any disturbance. When bringing the memory to mind, you will feel calmer and you will have a more adaptive response to yourself, which may take the form of positive beliefs about yourself, greater self-acceptance, and / or more confidence and self-compassion.
You will still be able to retrieve the memory, but it will not disturb or bother you any longer.
Can I do EMDR Myself (or to someone else)?
NO – A common question clients have is whether they can simply “move their eyes left-to-right” while thinking of a painful memory and process that memory themselves. This is not advised (and is potentially unsafe) for several reasons:
Firstly, an EMDR Therapist must undergo a minimum of 50 hours training comprising of: 20 hours of didactic training, 20 hours of skills training and 10 hours of consultation with an EMDRAA Accredited Consultant. Part of this training encompasses understanding the numerous components of an unprocessed memory and how they interact (images, sounds, smells, bodily sensations and negative views of Self), what decisions to make whilst processing memories (EMDR Therapists do not just ask you to move your eyes back and forward – at each stage of processing, they are actually looking for specific cues from you that the individual components of the memory are being successfully processed, before they move onto the next memory component), and how to determine that a memory has indeed been successfully (and safely) processed.
As you can see, each of these components is complex and cannot be executed by one’s self, on one’s self. Similarly, before memory processing can commence, an extensive history must be taken by the therapist to determine the themes, patterns, and cautions that need to be kept in mind when doing memory processing. These skills require professional objectivity, extensive university training, and clinical experience. You cannot do these things yourself.
Secondly, it is not possible to take one’s self through the steps of memory processing because they are so complex that it would not be possible to fully stay ‘in a memory’ whilst self-monitoring. This means you cannot be processing a memory AND be consciously maintaining awareness of (and fidelity to) the EMDR Treatment Protocol (the decision-making steps based on responses made after each set of eye-movements). In other words, even if you knew what the steps were to processing a memory, you would not actually be sufficiently ‘present’ and engaged in your memory – if you were simultaneously mentally taking yourself through these steps – to derive any benefit from doing any EMDR to yourself. EMDR Therapy may appear simple, but unfortunately, it is not something you can do, yourself.
Third, often processing a memory may bring you to the edge of your Window of Tolerance. An EMDR Therapist is trained to help you recognise the cues that this may be happening, and is trained to work with you to ensure that you can keep processing memories, safely. This is not possible (and may be harmful) if you try to perform EMDR with yourself (or anyone else). You may even cause a negative emotional reaction that you cannot manage, and this could put you (or another person) at risk of re-traumatization, dissociation, or self-harm. If this happens, chances are that is not something that you have skills or training to manage.
Think about it this way – Therapists who know how to do EMDR Therapy very well STILL go and seek the help of an EMDR therapist when they have memories that need to be processed. This is because EMDR Therapy requires a therapist to guide the process.
Similarities & Differences Between Other Approaches
Cognitive-Behaviour Therapy (CBT): We all can have negative thoughts and negative Self Beliefs. However, whereas CBT focuses on homework exercises designed to help you challenge all negative thoughts with the expectation that emotional changes come from helping you ‘think differently’, EMDR Therapy has no homework and does not require you to ‘think differently’.
Rather, one of the many positive side-effects of having successfully reprocessed a difficult emotional experience using EMDR Therapy is that people spontaneously report that their negative Self-Belief has in fact been replaced with a more positive Self-Belief. In other words, one indication that an event has been successfully ‘resolved’ with EMDR Therapy is that a person endorses a more positive view. This happens every time an experience is reprocessed in the Treatment Stage of EMDR Therapy, WITHOUT the typical rationalizing or homework exercises characteristic of CBT.
Mindfulness: Mindfulness is a way of attending to experience (i.e., our internal and the outer world) from the perspective of a non-judgmental Observer. Although Mindfulness is not a treatment in itself, it is a hugely important skillset that can increase your capacity for self-awareness, for insights, and for tolerate strong emotions and challenging internal experiences. Unsurprisingly, the capacity to attend to one’s experience in this way is a hugely useful asset to bring to (or develop in) any therapy. (You can read more about Mindfulness in articles I have written: here and here.)
In the Resourcing Stage of EMDR Therapy, clients are often taught brief Mindfulness skills that can help increase self-awareness and objectivity which can be essential in helping people attend to their experience in ways that are helpful (vs harmful). In the Treatment Stage of EMDR Therapy (which incorporates bi-lateral stimulation) individuals are specifically asked to make use of Mindfulness to mindfully attend to all of their experience (thoughts, feelings, imagery, emotions, sensations in the body, and any other associations their mind may be making) and to objectively report their experience and observations which helps the therapist to understand what aspects of a reprocessing a past experience remain and to determine when it is time to move onto the next Stage of the Treatment.
Acceptance & Commitment Therapy (ACT): ACT is about helping you clarify meaningful and pragmatic (tangible) goals that are deeply connected to your values, and it aims to teach you Mindfulness and distress-tolerance skills so that you can be freer to take more workable actions in directions that serve you (even if discomfort is present). ACT is an ‘experiential therapy’ (the insights you gain come not from talking, but from the insights you gain via participating in ACT experiential practices).
Equally, EMDR Therapy (particularly in the Resourcing and Treatment Stages) make extensive use of Mindfulness and distress-tolerance skills. For example, in the Resourcing Stage, EMDR therapists trained in ACT may draw upon experiential exercises from ACT (to help increase your Window of Tolerance in preparation for the Treatment Stage). Equally, Treatment Stage in EMDR Therapy is also highly experiential and makes use of mindfulness and distress tolerance-skills commonly taught in ACT. In this way, EMDR Therapy can make use of ACT skills and is consistent with ACT: EMDR Therapy aims to help free you from your past, so that you can be free to choose how you respond and can live a freer and more valued-life.
However, whereas ACT focuses on increasing your distress tolerance so that you can ‘take action’ in important areas of your life that you were previously avoiding, with EMDR Therapy once you have re-processed the material underlying your difficulty it is often the case that there is no ‘distress’/’disturbance’ left to apply any skills to. This is a significant different between the approaches (i.e., ACT prepares you to handle distress as an end point, whereas EMDR Therapy aims to removes).
Compassion-Focused Therapy (CFT): Both EMDR Therapy and CFT make extensive use of soothing Imagery and Imagery Rescripting to change how you respond to internal experiences and life’s challenges. Both EMDR Therapy and CFT also result increased self-awareness and (most importantly) an increased capacity for individuals to respond to prior difficulties with a deep sense of Self-Compassion. (I have written articles about the benefits of Self-Compassion and common resistances people have to developing a self-compassionate stance, here.)
Psychodynamic Therapies: Psychodynamic Therapies (there are many variants) and comprehensive EMDR Therapy can focus on elements of the unconscious mind (including unresolved conflicts and repressed emotions) and past experiences as a way to help individuals understand and resolve their current psychological problems. Ideally (provided that your EMDR Therapist is highly skilled), EMDR Therapy can serve as a ‘complete treatment’ (vs just a ‘technique’); one that focuses on Early Childhood, Attachment, and Unmet Needs at all Stages (Assessment, Preparation, & Treatment Stages) to help you better understand the patterns that give rise to your current emotional difficulties (to which the EMDR Therapy is then applied).
In Psychodynamic Therapies and in in EMDR Therapy (and many modern contextual and behavioural therapies such as ACT and CFT) the relationship between yourself and your therapist is understood to serve as a possible window into the problematic relationship patterns in your life. Although historically this was a ‘defining characteristic of Psychodynamic Therapy’, nowadays most Psychologists are also trained to attend to the nature of the dynamic between you and this is certainly a focus in other therapies including ACT, and CFT discussed above. However, whereas in Psychodynamic Therapies the focus on this dynamic is often central to the ‘treatment’, in EMDR Therapy this element features most commonly in the Assessment, and Preparation Stages (i.e., in EMDR Therapy the Treatment Stage is focused on helping your brain heal itself).
Like Psychodynamic Therapies, the Treatment Stage of EMDR Therapy makes use of free association and this can extend to working with symbolic experiences (including memories, imagery and dreams). In addition, both therapies (provided EMDR Therapy is conducted by a highly skilled therapist) share a focus on exploring the nature of your relationships with others, including family members and Attachment figures, and how these relationships may have influenced your current psychological state.
However, a major difference is that: Whereas Psychodynamic Therapy is a purely ‘talking-therapy’ (the success of which is in-part determined by the accuracy of the interpretations of your therapist, combined with your capacity to develop insight based on these interpretations), in the Treatment Stage of EMDR Therapy there is very little talking done at all. Rather, it is via the systematic (i.e., focused) eliciting of the specific components we know from the decades of research to underlie each element of an unprocessed emotional experience in conjunction with bi-lateral stimulation and free association. This can be combined with Imagery Rescripting, to help you work with your brain’s representation of the earliest developmental experiences.
Does EMDR Therapy Work Online (via Telehealth) ?
YES! There is strong evidence supporting the effectiveness of EMDR Therapy delivered online. The Covid-19 pandemic spawned dozens of studies into the effectiveness of EMDR Therapy delivered online versus in-person. This research finds online EMDR Therapy is just as effective. and we can say this with a high degree of confidence. Below, you’ll find a compilation of peer-reviewed research publications validating this claim. Recommendations for online EMDR Therapy include: Ensuring the use of a hands-free device with a sufficiently large screen to facilitate the required left-to-right eye movements for bilateral processing. Additionally, it’s essential to have a quiet and private location for memory processing sessions, free from potential disruptions such as people, pets, or device notifications.
Research on the Effectiveness of Online EMDR Therapy
Bates, A., Rushbrook, S., Shapiro, E., Grocott, M., & Cusack, R. (2020). CovEMERALD: Assessing the feasibility and preliminary effectiveness of remotely delivered eye movement desensitisation and reprocessing following Covid-19 related critical illness: A structured summary of a study protocol for a randomized controlled trial. BioMedCentral, 21: 929. Open Access: https://doi.org/10.1186/s13063-020-04805-1
Bongaerts, H. Voorendonk, E. M., van Minnen, A., & de Jongh, A. (2021). Safety and effectiveness of intensive treatment for complex PTSD delivered via home-based telehealth. European Journal of Psychotraumatology, 12(1), 1860346. Open access: http://dx.doi.org/10.1080/20008198.2020.1860346
Bursnall, M., Thomas, B. D., Berntsson, H., Strong, E., Brayne, M. & Hind, D. (2022). Clinician and patient experience of internet-mediated eye movement desensitisation and reprocessing therapy. Journal of Psychosocial Rehabilitation and Mental Health, 28. Open access: https://doi.org/10.1007/s40737-022-00260-0
Lazzaroni, E., Invenizzi, R., Fogliato, E., Pagani, M., & Maslovaric, G. (2021). Coronavirus disease 2019 emergency and remote eye movement desensitization and reprocessing group therapy with adolescents and young adults: Overcoming lockdown with the butterfly hug. Frontiers in Psychology, Psychology for Clinical Settings, 701381. Open access: https://doi.org/10.3389/fpsyg.2021.701381
Lenferink, L. I. M., Meyerbroker, K., & Boelen, P. A. (2020). PTSD treatment in times of COVID-19: A systematic review of the effects of online EMDR. Psychiatry Research, 293:113438. Open access: https://doi.org/10.1016/j.psychres.2020.113438
Liou, H., Lane, C., Huang, C., Mookadam, M., Joseph, M., & Hecker DuVal, J. (2022). Eye movement desensitization and reprocessing in a primary care setting: Assessing utility and comparing efficacy of virtual versus in-person methods. Telemedicine and e-Health, Ahead of Print. https://doi.org/10.1089/tmj.2021.0454
Marotta-Walters, S.A., Jain, K., DeNardo, J., Kaur, P., & Kaligounder, S. (2018). A review of mobile applications for facilitating EMDR treatment of complex trauma and its comorbidities. Journal of EMDR Practice and Research, 12(1), 2-15. Open access: http://dx.doi.org/10.1891/1933-3196.12.1.2
McGowan, I. W., Fisher, N., Havens, J., & Proudlock, S. (2021). An evaluation of eye movement desensitization and reprocessing therapy delivered remotely during the Covid-19 pandemic. BMC Psychiatry, 21, 560. Open access: https://doi.org/10.1186/s12888-021-03571-x
Mischler, C., Hofmann, A., Behnke, A., Matits, L., Lehnung, M., Varadarajan, S., Rojas, R., Kolassa, I-T., & Tumani, V. (2021). Therapists’ experiences with the effectiveness and feasibility of videoconference-based eye movement desensitization and reprocessing. Frontiers in Psychology: Psychology for Clinical Settings, 748712. Open access: https://doi.org/10.3389/fpsyg.2021.748712
Moench, J., & Billsten, O. (2021). Randomized controlled trial: Self-care traumatic episode protocol (STEP), computerized EMDR treatment of COVID-19 related stress. Journal of EMDR Practice & Research, 15(2), 99-113. http://dx.doi.org/10.1891/EMDR-D-20-00047
Perri, R. L., Castelli, P., La Rosa, C., Zucchi, T., & Onofri, A. (2021). COVID-19, isolation, quarantine: on the efficacy of internet-based eye movement desensitization and reprocessing (EMDR) and cognitive-behavioral therapy (CBT) for ongoing trauma. Brain Sciences, 11(5), 579. Open access: https://doi.org/10.3390/brainsci11050579
Perez, M. C., Estevez, M. E., Becker, Y., Osorio, A., Jarero, I., & Givaudan, M. (2020). Multisite randomized controlled trial on the provision of the EMDR integrative group treatment protocol for ongoing traumatic stress remote to healthcare professionals working in hospitals during the Covid-19 pandemic. Psychology and Behavioral Science, 15(4), 555920. DOI: 10.19080/PBSIJ.2020.15.555920. Open access: https://juniperpublishers.com/pbsij/PBSIJ.MS.ID.555920.php
Spence, J., Titov, N., Johnson, L., Dear, B. F., Wootton, B., Terides, M., & Zou, J. (2013). Internet-delivered eye movement desensitization and reprocessing (iEMDR): An open trial [version 2; peer review: 2 approved]. F1000Research, 2:79. Open access: https://doi.org/10.12688/f1000research.2-79.v2
Tarquinio, C., Brennstuhl, M., Rydberg, J. A., Bassan, F., Peter, L., Tarquinio, C. L., & . . . Tarquinio, P. (2020). EMDR in telemental health counseling for healthcare workers caring for COVID-19 patients: A pilot study. Issues in Mental Health Nursing, published online. Open access: https://doi.org/10.1080/01612840.2020.1818014
Todder, D., & Kaplan, Z. (2007). Rapid eye movements for acute stress disorder using video conference communication. Telemedicine and e-Health, (13)4, 461-464. http://doi.org/10.1089/tmj.2006.0058
Winkler, O., Dhaliwal, R., Greenwhaw, A., O’Shea, K., Abba-Aji, A., Chima, C., Purdon, S. E., & Burback, L. (2021). Web-based eye movement desensitization and reprocessing for adults with suicidal ideation: Protocol for a randomized controlled trial. JMIR Research Protocols, 10(11): e30711. Open access: https://doi.org/10.2196/30711
If you have further questions about how EMDR Therapy can help you to get past your past, please contact me below.
I am PhD Clinical Psychologist with over 15 years experience. I am an Accredited EMDR Practitioner.
Summary
EMDR Therapy is a very unique and powerful approach to resolving painful memories that was originally developed to treat trauma, over 30 years ago
EMDR Therapy has far-reaching applications beyond large or obvious traumas and is essentially useful to consider whenever the past is causing an individual significant disturbance and/or a negative view of themselves.
Present day stress and triggers exist because of unprocessed memories from our past.
Early painful attachment experiences and Adverse Childhood Experiences(ACEs) are examples of developmental experiences that may leave a lingering effect on an individual, and these may be useful to work on using EMDR Therapy.
In EMDR Therapy, the therapist takes each of the stuck components of an unprocessed memory and uses the bilateral stimulation to help the brain store this information in new ways. In doing so, the information from the memory is transferred from the limbic system to the pre-frontal cortex where a person can make better sense of what has happened. This leaves a person feeling resolved (vs ‘stuck’) about the corresponding memory and its components.
Preparation involves: Taking a History, determining your Present Triggers and Future Goals, mapping your memories into themes, establishing your Window of Tolerance, and building skills so that you can handle any difficult emotions that may show up as when you bring up the memories that are affecting you.
During a memory-processing session, a client is asked to recall specific components of the problem memory as directed by their therapist – this may include its image, the negative self-belief, and/or the disturbing emotions and associated body sensations. This happens while simultaneously engaging in bilateral stimulation (i.e., stimulation involving both sides of the body) such as left-to-right eye movements (or bi-lateral sounds, flashing lights, or ‘tapping’).
Eye movements are the most common bilateral stimulation used and these are believed to mimic the eye movements of REM sleep (the stage of sleep responsible for memory processing and learning).
These eye-movements may be repeated quickly, in sets of 20-30 (several times), until processing has completed.
EMDR Therapy is very different to regular ‘talking therapy’ – During processing a memory, there is very little talking (other than a brief ‘check in’) in between the bilateral stimulation
Processing a memory can happen very quickly (in as little as a single session)
Due to the Generalisation Effect, you do not need to process every single memory – processing one event or memory may also help reduce the disturbance you experience in response to similar memories.
EMDR Therapy can be highly effective when delivered online, but working with trauma requires extensive and advanced supervised training to ensure that it is a safe and comfortable experience. Therefore, you should not attempt to perform EMDR Therapy (on yourself or anyone else) because this could become highly unsafe.
I am a PhD Clinical Psychologist and EMDR Accredited Practitioner with over 15 years of psychotherapy experience. Whether you are seeking an assessment and diagnosis, or are searching for integrative research-backed ways to help you heal past wounds, break reactive-patterns and achieve long-lasting change, my aim is to provide a safe space for you to feel seen, understood, and empowered so you can make meaningful progress on your healing journey.
I endeavor to reply to all enquiries within 24 hrs.
About Me:
Dr Andreas Comninos, PhD Clinical Psychologist
I am a PhD Clinical Psychologist and EMDR Accredited Practitioner with over 15 years of psychotherapy experience. Whether you are seeking an assessment and diagnosis, or are searching for integrative research-backed ways to help you heal past wounds, break reactive-patterns and achieve long-lasting change, my aim is to provide a safe space for you to feel seen, understood, and empowered so you can make meaningful progress on your healing journey.
Attachment is an evolutionary model that explains how humans develop and function in relationships across the lifespan. Attachment science is one of the most researched areas in psychology. Its history spans over 60 years of research in humans alone, and many decades of research in animals prior (eg, from Lorenz’s observations of imprinting in newborn ducklings in the 1930s, to Harlow’s studies of the effects of maternal deprivation on infant primates in the 1950s).
Essentially, our ‘Attachment Style’ is formed in response to the emotional quality of the relationship provided to us by our primary caregivers. We know that early attachment experiences strongly influence human development in many key areas, including how our brains and immune systems develop, how we learn to self-regulate in response to both pleasant and unpleasant events, and how we learn to experience and communicate our emotions (and needs). As adults, our attachment experiences inform our perception and understanding of relationships and this heavily influences how we are likely to feel and behave in relationships, why we choose the partners we choose (and/or why we choose emotional distance from others).
This page aims to provide you with a deeper appreciation of how Attachment Styles develop and how they affect your current functioning. Early attachment experiences organize the internal worlds of us alland this influences the majority of our relationships (including our relationship with ourselves). Therefore, this a hugely important topic that deserves your time, attention, reflection and care.
Because neglect, parental inconsistency and a lack of love (experienced or perceived) can lead to long-term mental health problems as well as reductions in overall human potential and happiness, it is hugely important to learn about how our attachment experiences have shaped us, and for us to consider working towards healing our past attachment wounds. For many, there is truth to the anecdote: “We spend the first 15 years surviving living with our family and the rest of our lives healing from it”.
Not only do our attachment experiences shape how we are in relationships, they also extend to how we treat ourselves – this includes our ability to notice when we are suffering and also our response to our emotional needs (or why we may have learned to be insensitive to our emotional needs). This ‘responsiveness to Self’ (or a lack thereof such as when we are turning away from ourselves) is heavily influenced by what was (and often what was not – but should have been) taught to us by our primary attachment figures.
What is Attachment?
Our earliest attachments with parents or caregivers shape our abilities and expectations for relationships throughout life. The quality of our bond within these early relationships influences how our brain and immune system develops, how our sense of Self develops, and it also explains how we learned (or why did not learn) to regulate our emotions. The quality of our bond within these early attachment relationships also influences how we strive to satisfy our desire for closeness (vs independence), how we believe relationships work, and what we expect from our partners.
Attachment styles help explain how people respond differently when dealing with challenges of:
Uncertainty or distress
Strong emotions (negative and positive)
General setbacks (and how we relate to failure)
Understanding and communicating emotions (yours & the emotions of others)
Making ‘bids for emotional intimacy
Eliciting ‘care’ from others & responding to this care
Communicating expectations within a relationship
Identifying and communicating needs (your own and your partner’s)
Conflict & emotional disconnection
So, a person’s attachment style first forms in childhood, and then serves as a model for navigating life and relationships in adulthood.
How Attachment Develops
Early in life, humans are predisposed to focus on learning about other people’s reactions and how our behaviour can affect others. As infants, we are completely dependent on our caregivers for food, shelter and affection. As a survival mechanism, our brains have evolved to be very focused on establishing connection, whilst being highly sensitive to disconnection.
The effects of our early attachments with parents or caregivers can trigger a cascade of changes genetically, cognitively, socially, and physically which can have either positive or negative lifelong consequences.
Unsurprisingly, early attachment experiences affect our relationship with ourselves (how we view and relate to ourselves during moments of difficulty) and our relationships with others (the partners we choose – or avoid – and the interpersonal patterns that we keep repeating with all others).
Essentially, this is because the same motivational systems that gave rise to the close emotional bond between parents and their children is responsible for the bond that develops between adults in emotionally intimate relationships.
Although our early attachment experiences do not necessarily have to define us, they set us up with a ‘template for relating’ to Self and Others, which ultimately becomes either an asset or risk factor in terms of our resilience to stress. We now know from decades of research that early attachment experiences heavily influence an adult’s susceptibility to mental health difficulties.
Still Face Experiment
The infamous ‘still face experiment’ (developed by Dr Ed Tronick in the 1970’s) is a powerful demonstration of a child’s need for connection and how vulnerable we essentially all are to the emotional or non-emotional reactions of our primary caregivers. This experiment gives us insight into what it is like when connection does not occur.
Non-emotional reactions are a signal of ‘disconnection’, which triggers a range of instinctual behaviours in an infant. The ‘still face experiment’ illustrates the effects of perceived ’emotional disconnection’ and demonstrates how vulnerable we all are to emotional connection (and disconnection) from our primary caregivers, be they male or female.
Although the ‘still face’ may seem like a trivial example, as you may be able to appreciate, as a child develops there are many complex factors at play between them and their caregiver that will continue to shape and to ultimately teach a child about emotion regulation and self-soothing, how to connect emotionally, and how to elicit care (including a child’s experience and expectations of care as being ‘available and helpful’).
Fathers are important too
Although the ‘mother-infant-bond’ is often cited as hugely important, we also know that the quality of a father’s bond and their emotional responsiveness is also hugely important to a developing child.
Notice how infants demonstrate the same connection-seeking behaviours to their fathers that the infants did with their mother in the previous video. Also, notice how these infants react just as strongly to their father’s ‘still’ face.
Again, understand that these connection-seeking behaviours and their associated reactions demonstrate an innate survival mechanism that is strongly influenced and shaped through parent-child interactions early in our lives. This ultimately informs how, when, why (and with whom) we seek (or avoid) connection as adults:
Although these are just very brief demonstrations, imagine the longer-term effects – over many years – of repeated parental unresponsiveness on the emotional development of an infant. Clearly, over time this would affect a child’s sense of safety and being their sense of feeling ‘cared-for’ by that parent. They may also go on to develop extremely negative views about themselves (such as ‘I do not matter’ or ‘I am unlovable’).
Unsurprisingly, research has shown that children who have parents who are not responsive to their needs have more trouble trusting others, relating to others, and regulating their own emotions.
Why do parents get it wrong?
Even for parents who want the best for their children, there are many reasons why they may struggle to be emotionally present in Secure Attachment ways with their children. For example, if you had a parent who was not responsive to your needs (was not Secure in their attachment style), or who may have even punished you for having certain emotions, you may struggle with knowing how to be Secure in your Attachment yourself. As a parent, you may have difficulties with emotion regulation or other emotional awareness ‘blind-spots’ that lead you to repeating behaviours similar to what you were exposed to with your own children.
At other times, parents lack the information about how attachment affects a child’s developing brain, or they may hold cultural (or outdated) beliefs about emotions and / or parenting that downplay the importance of maintaining an emotionally responsive connection with their children. Alternatively, some parents have strong dysfunctional beliefs about their own abilities (e.g., “I am a failure”) which can interfere with them being able to form a strong bond with their children. These are all common reasons why creating a Secure Attachment fails to occur.
On the other hand, there are also more complex challenges to developing Secure attachment. In households with children who are experiencing behavioural or other developmental difficulties, often parents become preoccupied with caring for that child to the detriment of the needs of other siblings. In households with divorce or a death of a parent there can be ruptures in the Attachment bond. In situations where there is domestic violence, it may be difficult (or unsafe) to show emotions. Unfortunately we know that people who were exposed to the following adverse childhood events (ACEs) can have difficulties with Attachment. Often these people had parents who were exposed to similar adverse events themselves (this is called intergenerational trauma).
We also know that drug and alcohol use can also negatively impact on emotional availability (and both intoxication and the resulting hangover can blunt emotional expression). Some parents have head injuries or other illnesses that make it difficult to show appropriate emotional reactions. Understandably, parents experiencing significant mental illnesses may also struggle to engage with their children in ways that cultivate a Secure Attachment bond.
However, there are also more common forms of disconnection that affect us all. Technology and ‘screen time’ has become a major part of our busy lives and nowadays it is not uncommon to see parents disconnecting from their children in the same ways that were demonstrated in the videos above, by simply using their phone.
For those who are interested, the following video captures what it is like for babies of parents who are immersed in their phones. Notice how absorption in a device triggers exactly the same response in a child as the parental complete non-responsiveness in the previous videos:
A Word of Caution !
Before you go down the road of using Attachment to blame or shame yourself (or your partner, if you are having relationship difficulties) please understand that: Attachment styles are ADAPTIVE behaviours from an earlier stage of life based on our upbringing. Although these behaviours may no longer serve us, they may be carried forward into adulthood. In other words, a child who is taught that relationships are untrustworthy or even frightening naturally learns to have SELF-PROTECTIVE behaviours in all of their relationships. This is not our fault – and it is completely understandable from a survival instinct perspective (after all, all humans are born completely dependent on their parents for food, shelter, nourishment, love and protection). However, as adults it is our responsibility to understand and heal from our childhood attachment conditioning, to help ourselves recognise that the past is affecting us and to provide ourselves with options (and the permission) to change and replace patterns that are no longer serving us.
Also, when considering your childhood attachment history, please keep in mind that parents do not necessarily have to be ‘highly abusive’ to have a negative effect on their children. Parents who are over-protective and intrusive, who are judgmental and have high expectations, or who are dismissive of a child’s thoughts and feelings can (over time) also cause a distrust of relationships – or even a distrust of a child’s own emotions – well into adulthood for that individual.
So in other words, if you learned in childhood that relationships are conditional, shaming, unstable, threatening, withdrawing or rejecting, it may cause you to be uncertain about relationships and this may lead to behaviours typical of the three non-secure attachment styles (anxious, avoidant, or disorganized behaviours). This is not your fault. These emotional reactions and their resulting protective behaviours are an understandable adaptive response to feeling insecure (or unsafe) in an important relationship during a critical stage of our development.
In other words, whereas being able to view attachment behaviours as ‘protective strategies from an earlier part of life that no longer serve us’ is crucial to our liberation, shaming or ridiculing ourselves (or our partner) for having attachment difficulties is probably doing nothing more than continuing to perpetuate the intergenerational toxicity that was handed down to us (or them) by caregivers. This is unlikely to result in freeing ourselves from these patterns and is more likely to continue to do further damage.
It is important to seek help for attachment difficulties. They are not easily resolved with self-help material alone. This is because attachment is relational, it involves your brain’s development and emotional learning in the context of interactions with others. There is learning, reflection, and healing that requires an emotionally-attuned and and emotionally-safe therapeutic environment, and there are skills that need to be honed and practiced interpersonally that cannot be mastered alone.
The Four Attachment Styles
The four attachment styles were born out of the seminal work of psychologists John Bowlby and Mary Ainsworth. In the 1950s, Bowlby proposed that attachment is the product of evolutionary processes and that infants are thus born with an innate drive to form attachments with caregivers. In the 1970s, Ainsworth developed a paradigm (the ‘Strange Situation’) to determine attachment security in children within the context of caregiver relationships. The ‘Strange Situation’ procedure involves series of eight interactions lasting approximately 3 minutes each, whereby a mother, child and stranger are introduced, separated and reunited. From this research, Ainsworth identified three main attachment styles (a fourth attachment style was later identified in the 1980s by psychologists Main and Solomon).
The four attachment styles consist of Secure Attachment and 3 Non-Secure Attachment Styles listed and described in detail with examples, below:
1) Secure
2) Anxious (aka Preoccupied)
3) Avoidant (aka Dismissive)
4) Disorganized
1. Secure Attachment:
Secure attachment is the ideal attachment style. Approximately 50-60% of adults have a Secure attachment style. A Secure attachment between a child and a caregiver forms when the caregiver is perceived as safe, predictable, consistent, and physically and emotionally available. The remainder of people develop one of three other attachment styles (Anxious, Avoidant or Disorganized, as discussed in the next section).
Secure attachments develop in the following ways: A securely attached infant believes her parent is safe, available, and responsive when she is in distress. Caregivers communicate these qualities the following ways: Facial expression, posture and tempo of body movement, tone of voice, physical proximity and tactile responsiveness, which together communicate a dependable, caring intention from the caregiver. (This is all pre-verbal information that an infant is constantly learning about and absorbing.) When a secure bond has been established, even the mere attention from or presence of a caregiver can help the infant to regulate distress.
As a result of a secure bond, even if the parent is not always available, the infant will learn to internalize these responses from their caregivers and they can draw on this internal representation to self-soothe and self-regulate during challenges or times of distress. As you can begin to see, this is essentially the origin of where we learn (or sadly where we fail to learn) emotional regulation.
Children with a secure attachment see their parent as a secure base from which they can venture out and independently explore the world. When a caregiver is emotionally responsive and strives to meet an infant’s emotional needs with consistency, the infant is taught to be emotionally responsive themselves. Thus, securely attached children grow into resilient, emotionally healthy adults who enjoy emotionally healthy relationships because they generally feel trusting and safe in those relationships.
In intimate relationships, a secure adult feels secure in their connection with their partner (even in their partner’s absence). This allows each partner to live their lives freely (which is called interdependence). Because a Secure individual is aware of and is able to respond in emotionally healthy ways to their own needs, this frees them up to be supportive at times when their partner feels distressed. Also, because a secure adult feels comfortable eliciting care from others, they are more likely to turn toward (vs shutting down or withdrawing from) their partner when they feel troubled.
In other words, an intimate relationship with a secure partner tends to be honest, open and equal, with both parties feeling independent, yet loving toward each other. Because of this, it is unsurprising that we find that compared to the other attachment styles, securely attached adults (and their partners) report feeling the highest levels of relationship satisfaction.
People with a secure attachment style:
Generally feel close to others
Feel comfortable with emotional and physical intimacy, and also with independence
Communicate effectively and resolve conflicts as they arise
Have fairly stable relationships
Generally trust in their partner
Feel safe in being vulnerable with their partner
Secure Attachment Example
A fantastic example of what Secure Attachment ‘looks like’ in the context of healthy (mutually secure) adult relationships is clearly evident in the (now) infamous “A Credo for My Relationships With Others“ by Clinical Psychologist Dr. Thomas Gordon. As you read through this Credo, I invite you to reflect upon whether you are achieving something like this within your important primary relationships (and if you are, reflect inwards about whether your are achieving this same harmony and respect internally – between the competing aspects of yourself):
A CREDO FOR MY RELATIONSHIPS WITH OTHERS
You and I are in a relationship which I value and want to keep. Yet each of us is a separate person with our own unique values and needs and the right to meet those needs.
So that we will better know and understand what each of us values and needs, let us always be open and honest in our communication.
When you are having problems meeting your needs, I will listen with genuine acceptance and understanding so as to facilitate your finding your own solutions instead of depending on mine. And I want you to be a listener for me when I need to find solutions to my problems.
At those times when your behavior interferes with what I must do to get my own needs met, I will tell you openly and honestly how your behavior affects me, trusting that you respect my needs and feelings enough to try to change the behavior that is unacceptable to me. Also, when some behavior of mine is unacceptable to you, I hope you will tell me openly and honestly so I can try to change my behavior.
And when we experience conflicts in our relationship, let us agree to resolve each conflict without either of us resorting to the use of power to win at the expense of the other’s losing. I respect your needs, but I also must respect my own. So let us always strive to search for a solution that will be acceptable to both of us. Your needs will be met, and so will mine—neither will lose, both will win.
In this way, you can continue to develop as a person through satisfying your needs, and so can I. Thus, ours can be a healthy relationship in which both of us can strive to become what we are capable of being. And we can continue to relate to each other with mutual respect, love and peace.
Dr. Thomas Gordon (1978)
Non-Secure Attachment Styles
2. Anxious Attachment (aka Preoccupied):
Children who had parents who at times responded well to their needs, yet at other times, were not emotionally present or may have responded in hurtful or critical ways, grow up feeling insecure, uncertain of what treatment to expect.
In relationships, adults with an anxious attachment style find that they need a lot of reassurance and responsiveness. Unlike a securely attached person, those with an anxious attachment style may appear overly dependent on their relationships to feel okay. Certain interactions or events may trigger deep mistrust and they may regularly feel heightened anxiety about the stability of their relationships.
Even though anxiously attached individuals may feel desperate or insecure, more often than not, their behaviour exacerbates their own fears (via a feedback loop called a ‘self-fulfilling prophecy’). They may also interpret independent actions by their partner as affirmation of their fears. Worse, when they feel unsure of their partner’s feelings or feel insecure in their relationship, they may become clingy, demanding or possessive toward their partner.
Although these are simply attempts to protect the Self via seeking a sense of safety, reassurance and security, by clinging to their partner or by engaging in behaviours called ‘Protest Behaviours’ a person with an anxious attachment style may unwittingly push their partner away. For example, if (say) a partner starts socializing more with friends, they may think, “See? He doesn’t really love me. I was right not to trust him – Maybe there is someone else… This means he is going to leave me.” This may lead to (for instance) lots of reassurance seeking behaviours, such as calling, texting, or even stalking or reading a partner’s private messages. Alternatively, it may lead to hostility towards that partner, who often will not understand the context of the person’s behaviour, and this may drive them away – particularly if the partner has an avoidant attachment style (below).
People with an anxious attachment style:
Feel the need for lots of reassurance in a relationship
Often report feeling overwhelmed or extremely anxious when they and a loved one disagree or argue
Question their partner’s love (e.g., especially at times when their partner is away)
Feels threatened by their partner needing a break (and may pursue them until they give in)
3. Avoidant Attachment (aka Dismissive):
Children of caregivers that were emotionally unavailable, absent, or unaware of their needs often develop an Avoidant attachment style. Perhaps crying was discouraged, or perhaps you were belittled for having emotional needs. As an adult, you may feel uncomfortable depending on someone, or being depended on by others.
A person with an avoidant attachment style lives in an ambivalent state, in which they are afraid of being both too close to and too distant from others. In relationships, they have fears of being abandoned but also struggle with being intimate. They may cling to their partner when they feel rejected, then feel trapped (or resentful, as though they will lose their sense of ‘Self’) if they become too emotionally intimate / close.
Often, in relationships, the avoidant style is attracted to the anxious style, and this sets off a push-pull between one partner (the anxious style) feeling unloved and the other partner (the avoidant style) feeling unable to meet the emotional demands of the other.
People with an avoidant attachment style:
Feel the urge to pull away when their partner is seeking connection or is distressed
Regularly feel emotionally removed from others
Want to distance themselves from (vs resolve) stressful situations or conflict
Are generally uncomfortable with their emotions. Partners often accuse them of being distant and closed off, rigid and intolerant. In return, they may accuse partners of being too needy.
May prefer fleeting, casual relationships to long-term intimate ones, or may seek out partners who are equally independent (or who will keep their distance emotionally).
If you have an Avoidant Attachment Style, it is important to respect (and be able to communicate) your needs for space in a relationship. One way of doing this is to use phrases that contain elements like: “This is not a reflection of how I feel about you – this is something that I need”.
Eg “I’m sorry – I am not feeling very communicative right now. But please understand that my not wanting to text message with you right now [or insert the specific action] is not a reflection of how I feel about you. Would it be OK if I do ‘me’ for a bit and I promise we will do something together later?”
By developing ways to express your feelings and needs clearly and warmly, and in ways that reassure your partner, they will understand you and will feel secure enough in your relationship to give you the space that you need. In turn, this sense of space will give you a sense of freedom and ‘security’ which will allow you to continue your connection with them – without feeling the need to cut it off to ‘survive’.
4. Disorganized (unresolved) Attachment:
Disorganized attachment is the primary style common in survivors of complex developmental trauma (cPTSD). For instance, perhaps a caregiver was frightening, abusive, or behaved in highly inappropriate ways; perhaps a child’s human rights were violated. These traumas can cause fear of a parent and/or deep confusion in a child (remember – human children are born dependent on their caregivers for nurturance, safety, shelter, sustenance etc) will develop the understanding that a parent is not present for them. However, this creates an internal dilemma: A child is completely dependent on their parent for food, safety and shelter. Often, a child’s innate desire for parental love may create an inner conflict whereby they believe that the behaviour of the abusive parent is their own fault, or that they should remain loyal because “they are my parents”. As an adult, a person with a disorganized attachment style may long for closeness, but may also fear it. They may not seek out relationships because they may feel like counting on others is unsafe. When presented with opportunities for closeness, they may pull away.
People with a disorganized attachment style:
May have had primary caregivers that were abusive (physically, emotionally, sexually, neglect etc)
Commonly report craving emotional intimacy, but also feel it is safer to be alone
May have had primary caregivers who showed love one minute but who were frightening the next
May have Complex Trauma (cPTSD)
May have a deep mistrust of others or question their positive intentions
Attachment & Emotion Regulation
Emotion regulation is the process by which we influence how we experience and express our feelings (which emotions we have, when we have them, and how they are expressed). Throughout our lives, emotion regulation is an important regulator of interpersonal relationships and in our relationship with ourselves.
The ability to regulate one’s emotions is taught in one’s earliest relationships. We are taught ‘how’ to feel (and we are often not taught how to feel) by our primary caregivers, and this becomes ingrained throughout childhood, and practiced throughout life. Thus, emotion regulation and quality of an infant’s attachment are closely linked.
In infants, patterns of emotion regulation are shaped and developed in direct response to experiences with their caregivers. Because an infant is dependent on a caregiver (e.g., for food, shelter, and protection), an infant’s emotional regulation serves the important function for the infant of maintaining a close relationship with the attachment figure. This ensures that the parent will remain close to the child and the child will thereby (hopefully) be protected. As was demonstrated in the “Still Face” videos above – this is a survival instinct (we are hard-wired to do this).
Therefore, it is easy to understand how infants of non-secure parents, who may experience repeated rejection, or hostility, may learn very quickly to minimize their own negative affect (i.e., by emotionally withdrawing or shutting down) in order to avoid the risk of further rejection. Often, infants internalise the voices of their parents – and this can lead to an internalisation of this response to self that persists into adulthood in the form of negative self-beliefs and/or self-criticism.
On the other hand, it is easy to understand how infants of mothers who have been relatively inconsistently available may maximize negative their affect in order to increase the likelihood of gaining the attention of a frequently unavailable caregiver. If this strategy succeeds, it becomes engrained through repetition as a natural response whenever faces with a similar situation. Clearly, this could result in difficulties with emotion regulation for the child that may persist into teenage years and adulthood.
Again, both of these patterns of emotion regulation are simply examples of primal attempts by the infant to remain in positive connection with the caregiver. When these patterns work, they are repeated and they become deeply learned emotional responses – ways that we may still strive to have our emotional needs met as adults.
The early experiences you had with your primary caregivers ALSO play a direct role in the development of your brain, which in turn influences your ability to regulate your emotions. Insecure or inconsistent styles of attachment result in the experience of feeling overwhelmed and unsafe in a child, which creates either Hyperarousal (being on high alert) or Hypoarousal (becoming numb) as means of protection. Left unaddressed, this can persist across the lifespan and can greatly affect adult relationships, including our relationship with ourselves.
Over time, these learned protective behaviours can reorganise a child’s brain during a particularly crucial stage of development (0-15 years) and this, in conjunction with either adverse childhood experiences, skills deficits, or maladaptive coping strategies, can lead to difficulties with emotion regulation in adults (such as a reduced Window of Tolerance, discussed in detail here). Essentially this is because through interacting with an infant in a very critical period of brain development (especially between 0 to 12mths) the mother begins to teach and shape how to down-regulate negative emotions but ALSO how to up-regulate positive emotions (such as joy, interest, excitement, which are important for play-states and the development of the dopaminergic-reward system).
This is essentially what we as adults are ultimately required to do for ourselves, in terms of regulating our emotions (by calmly activating and deactivating our arousal) in response to the full range of events and challenges that we experience. This is depicted in a simple way in the following diagram (taken from my Window of Tolerance article, discussed in detail here):
Moreover, we know that the broader the range of emotions a child learns to experience (and respond to), the broader the range of emotions the adult will be able to understand, experience, and respond to (and understand, experience, and respond to in others).
For these reasons, it follows that, whereas skills for emotional regulation may come significantly easier to those who have grown up with secure attachment, emotional regulation can be more difficult to learn for those who grew up with inconsistent, unavailable or abusive caregiving. Nevertheless, the good news is that we can learn to work with (and heal) our wounded attachment systems, and regarding improving our emotion regulation – this essentially involves developing a new set of skills, which can be learned.
Effects on Relationships
Although it is possible to have differing attachments with different people in our lives (e.g., you may simultaneously feel Secure in your attachment with a best friend, Anxious in your attachment with your boss, and Avoidant in relation to a pesky neighbour), we all have one primary attachment style. Each person tends to rely more on this one style than the other styles of relating.
In fact, this primary attachment style is so fundamental to how we process and make sense of the world that we even dream according to our primary attachment style. In one study, participants completed established measures of attachment to determine which attachment style best characterized them. Then, raters who were blind to the test results, listened to the participants’ recollections of dreams (listening carefully for themes, key people and the relationships between them). Amazingly, raters were able to correctly categorize participants’ attachment styles with a very high degree of accuracy, simply based on the content of their dreams (!). This result as been replicated in similar research.
In the area of intimate relationships, both male and female adults seeking long-term partners often identify qualities of responsiveness consistent with Secure Attachment caregiving (such as warmth, attentiveness, and sensitivity), as the “most attractive” qualities in potential partners. Yet, as you are probably aware, despite the attractiveness of these secure qualities, not all adults are paired with secure partners.
This is because it is common for people to find themselves in relationships with partners who confirm their existing attachment experiences regarding relationships, care, and love. In other words, as adults we are subconsciously drawn towards partners who replicate the attachment dynamics that we experienced as children – even when these dynamics are not helpful for us.(This is because our ancient brains are drawn to this ‘familiarity’ on a primal, subconscious level).
However, this need not be the case. If you are in a relationship that contains unhealthy attachment dynamics, you can become aware of them and work with your partner (or with a therapist) to improve and change unworkable patterns. Or, if the dynamic is truly dysfunctional and toxic, you can work towards terminating an unworkable relationship.
Alternatively, if you are not in an intimate relationship (or if you are not seeking one), understanding your Attachment style is still hugely important because it strongly influences how you relate to yourself and communicate with (and understand) others.
It’s Not Your Fault
As discussed earlier, there are many reasons a parent may struggle to be emotionally present with their children. For the most part, most parents try as best as they can to deal with the challenges of parenting with the emotional regulation skills that they have, many of which were passed onto them by their own parents.
Unfortunately, children of parents who lacked the capacity to understand how what they are doing was ultimately affecting their child’s psychological growth and well-being, will most likely be those who have the deepest attachment wounds (and challenges managing relationships, including their response to emotions and needs of the Self). This is because, as humans, we have built-in survival instincts. As infants, our attachment style was our best means of self-protection.
If you align with a “non-secure” attachment style, it is not because you did something wrong. Rather, your attachment style results from surviving your upbringing. In other words, a ‘non secure attachment style’ is a response to this period because it was how we learned to “balance out” the challenges of the caregiving provided to us. Any non-secure attachment style we may develop was the best way we to could cope with the difficulties of circumstances we were handed. In other words, our attachment experiences are not our fault (!). We did not choose our families, nor did we choose the difficult early childhood experiences we were exposed to.
No matter which attachment style you currently have, know that secure attachment is possible. Learning about attachment is a journey of healing, self-compassion, and moving towards a more secure attachment style that will ultimately lead to healthier, more rewarding relationships.
You can recover from your attachment wounds. You can learn to develop new ways to relate to yourself and to connect with others. Learning about attachment by reading this article (and some of the articles at the bottom of this page) marks the beginning of this journey…
Healing Your Attachment Wounds
We now know that the attachment style you developed as a child based on your relationship with a parent or early caregiver does not have to define your way of relating to yourself, or to those you love in your adult life. In fact, we know that healing our attachment wounds is possible through heathy, emotionally corrective relationships.
We know that healthy attachment to others is our primary protection against feelings of helplessness and meaninglessness. For instance, close, connected relationships can actually reduce anxiety and fear by easing our primal fear of abandonment. This is because strong, attached relationships reduce feelings of fear (threat activation) and help “calm the brain”.
Whereas emotional isolation is more dangerous for health than smoking or a lack of exercise (e.g., people who live alone experience three times as many strokes as those who are married), those who feel the safety of a comforting relationship actually are more resilient in life and can go out and take more risks. Quite simply, loving and being loved makes one stronger. Those who have trust in each other can turn to each other in times of distress and this creates even more emotional safety.
Emotionally corrective relationships can be intimate relationships that you may have with a trauma-aware emotionally supportive partner (or a close friend) who either has a secure attachment style or who has done a lot of this work in therapy themselves. This person may be willing to hold space for you while also holding you accountable, as you work through the pain of your past together in all the ways that this may emerge within the dynamics of your relationship. Again, these individuals are often people who have often already done the work of therapy and have done the work of breaking their attachment patterns. However, these relationships deserve to be cherished and they are not a complete substitute for working with a professional who is trained in helping people heal from attachment wounds.
Unfortunately, for people with complex attachment wounds, developing a secure relationship with the ‘right kind of person’ who is emotionally safe, knowledgeable, patient, unconditionally non-condemning and capable of providing a consistent secure base is a huge task, and there will likely be many hurdles along the way. Attachment patterns can be very challenging to understand and very resistant to change, and this can put significant strain on relationships. Again, working with a professional who is trained in helping people heal from attachment wounds is highly recommended.
Although self-help information can be useful, it is also important to seek help for attachment difficulties and not to rely on self-help material alone. This is because attachment is relational, it involves your brain’s development and emotional learning in the context of interactions with others. The learning, reflection, and healing that is needed to address issues of attachment require an emotionally-attuned and emotionally-safe therapeutic environment in which to do this work, and to practice interpersonal skills that cannot be mastered alone.
Developing Secure Attachment
Seen, Soothed, & Safe = Secure Attachment
Secure Attachment can be BEST summarized with the concept of: ‘Seen, Soothed, & Safe’. Although this idea was initially developed by Dr. Dan Sigel (Neuropsychiatrist, Researcher, and best-selling Author) to help simplify Attachment for parents seeking to understand, attune to, and provide for their child’s emotional and developmental needs, the concept of Seen, Soothed, & Safe can be applied to two further areas: How we as adults relate to others and more importantly, how we relate to (and care for) ourselves.
Seen
‘Seen’ means to acknowledge and understand the mind, and emotions of another. This involves showing interest, empathy and curiosity about the feelings, perspectives and needs of another and being supportive an responsive to the emotional worlds of another person (it is the opposite of a dismissive parenting style that ignores, invalidates, or belittles a child for having the feelings or reactions that they might be having). It also requires being able to remain ‘present’ with and attuned to another person. This is not simply about eye-contact; it is about any actions you can take that may communicate to another person that you ‘get it’ at a ‘feeling’ level – that you truly understand their emotional experience. Mindfulness skills, Active Listening skills, and checking that you have heard what someone is saying correctly, can greatly help with this.
Appling ‘Seen’ to Ourselves: This means developing awareness of our own internal worlds, being able to identify, understand, and take responsibility for working with our emotions. It also means identifying and understanding what we need, and being interested and willing to respond to meeting those needs. If this learning was not provided to us by our primary caregivers, this may require therapy and practice.
Soothed
‘Soothed’ means to provide a sense of comfort and calm to another when they are experiencing difficult emotions or situations, in order to help settle and soothe their nervous system, to provide emotional support, or to provide a ‘space’ to be with the difficulty that they may be experiencing. Soothing may be enhanced by the ways we use our voice (tone, speed, expression), and/or physical gestures like body language, eye-contact, hand holding, or hugging.
Applying ‘Soothed’ to Ourselves: Being able to comfort and care ourselves by responding to our needs with healthy self-care actions, that support, settle, and soothe our nervous systems are all hallmarks of being able to provide a sense of ‘soothed’ to ourselves when we are having difficulties. This may require the prior development and practice of self-regulation skills learned in either therapy or via useful self-help tools.
Safe
‘Safe’ means to provide a sense of emotional availability and/or protection to others which can be demonstrated in a variety of ways, such as via the aforementioned ‘Seen’ and ‘Soothed’ actions, by being ‘present’ and attuned to their inner worlds and demonstrating that you can be a stable and dependable figure during in times of distress. Other actions that cultivate a sense of ‘safe’ may include: Being able to provide emotional a ‘space’ for others where they feel accepted when experiencing their difficulty, by being reliably accountable for one’s actions where there is a contribution to the difficulty (i.e, taking appropriate responsibility to ‘right a wrong’), and checking-in on how another person is feeling in a reliable and a consistent way.
Applying ‘Safe’ to Ourselves: In addition to the skills required to feel we are ‘seen’ and can ‘soothe’ ourselves, being able to communicate through our intentions and our actions that we can care for ourselves in healthy ways (no matter what we may be feeling) can provide a deeper sense that we are ‘safe’ within ourselves. This is largely achieved by being able to respond to our inner worlds consistently with care, acceptance and compassion. This demonstrates to us that ‘it is OK’ to feel what we are feeling. Being proactively responsive to our emotions and our needs (which may include taking assertive actions to elicit care from others) and assertive communication skills are additional resources that can contribute to our sense of ‘safe’.
The video below summarizes the above concepts. Although it presents them as ‘4’ separate elements, they are essentially just 3 because: Seen + Safe + Soothed = Secure Attachment.
Individual Therapy
A skillful trauma-informed psychologist who has undertaken the appropriate training can offer you the experience of a healthy, emotionally corrective relationship. Such a therapeutic relationship has the potential to be an emotionally corrective relationship partly because it is the therapist’s job to be ethical, consistent, and to build in security while being fully present for their clients.
The goal of therapy in providing a secure attachment is to model healthy ways to relate to others and to provide a safe environment for you to learn to attend to and express your own feelings and needs, while also healing past wounds and practicing new skills. In this way, you can work towards developing more secure ways of relating to others, often referred to as ‘Earned Secure Attachment‘. With the support of your therapist, you will be able to begin to apply these new strengths outside therapy in relationships that matter to you such as with a partner, children and friends. This work can take time – but it can be done whether you are in an intimate relationship, or not.
In terms of using the emotionally corrective relationship of therapy to improve your relationship with yourself (which is also an important part of developing ‘earned secure attachment’), this may involve learning new ways of being able to soothe and support yourself when you are struggling or are experiencing a setback – these emotional skills will likely not have been made available to you as a child. For people with significant developmental traumas (such as attachment wounds or Adverse Childhood Events), therapies such as EMDR Therapy may be useful in helping you to remove the disturbance of painful memories so that you can put your past behind you, and create the relationships with yourself and others that you ultimately were unable to have.
If you are troubled by memories that disturb you, or if you are tired of being emotionally triggered by events, I recommend reading my page about EMDR Therapy.
Attachment-Focused Therapy for Couples (EFT)
The most well researched therapy for couples that makes use of attachment science is called Emotionally Focused Therapy (EFT) for Couples. EFT for Couples is a short-term therapy that is aims to improve attachment and bonding in adult relationships. EFT for Couples is about creating connection in close relationships. It helps couples to understand and express their emotional experience including their needs, feelings, thoughts, and behaviours.
EFT for Couples is acknowledged as the gold standard for empirically validated interventions in tested interventions for couples. This research shows large treatment effect sizes and impressively, stable results over time.
EFT is the only model of couple intervention that uses a systematic empirically validated model of adult bonding (attachment) as the basis for understanding and alleviating relationship problems. Developed over 30 years ago by Sue Johnson, EFT for Couples is essentially attachment science in a therapy. As has been discussed, attachment science views human beings as innately relational, social and wired for intimate bonding with others. The EFT model prioritizes emotions and emotional regulation as the key organizing agents in individual experiences and key relationship interactions.
Below is a short video explaining research that Sue Johnson and her team performed, involving brain scans of people in relationships who were treated with EFT for Couples. It demonstrates how developing a strong relationship bond can reduce feelings of fear (threat activation) and can help “soothe the threatened brain”.
EFT for Couples not only addresses factors such as relationship distress, intimacy, trust, and the forgiveness of injuries, but it also aims to influence and heal you and your partner’s attachment style.
Emotionally Focused Therapy (EFT) involves discussing specific incidents that may occur in your relationship, as a way to help each of you learn about your emotions and the behaviours that result from those incidents.
For example, your therapist may discuss your partner reminding you to take out the rubbish and how that makes you feel. Do you feel angry? What else might you feel? Are you ashamed because you forgot, so that makes you want to lash out in anger? Do you feel judged as “not good enough” by your partner and that makes you feel as if you disappointed her? Does this then make you want to pull away from her?
Goals of EFT for Couples:
To create a positive shift in partners interactional positions and patterns.
To foster the creation of a secure bond between partners.
To expand and re-organize key emotional responses and, in the process, the organization of self.
If you are in a relationship in distress, or you would like to improve your relationship in any way, I highly recommend learning more about the work of Sue Johnson and finding a psychologist who can offer EFT for Couples.
A more in-depth presentation about Attachment and EFT for Couples:
Parents & Caregivers
If you are a parent whose childhood attachment experiences were less than ideal, or worse, perhaps you were exposed to significant traumas commonly referred to adverse childhood events (ACEs), I recommend that you engage in therapy with a clinical psychologist that is trauma-informed, and attachment aware (Please note: Sadly, not all psychologists are). Options for family therapy also abound.
It is also be important to invest in education. My recommendations are to undertake one (or both) of the following established and researched-backed programs:
An international program designed for parents and carers of children aged 0-12 years who want to strengthen the bonds with their children and would like support to help their children to build secure relationships. There is evidence that parents can in fact positively change a child’s insecure attachment style to ‘secure’ with COS training.
Collaborative and Proactive Solutions (CPS) training (external link)
CPS is an evidenced-based model of psychosocial treatment developed by Dr. Ross Greene, and described in his books Raising Human Beings, Lost at School, &The Explosive Child (another highly recommended ground-breaking approach to understanding and parenting children who frequently exhibit severe fits of temper and other significantly challenging behaviours).
Rather than focusing on kids’ challenging behaviours (and modifying them), CPS helps kids and caregivers solve the problems that are causing those behaviours. This problem solving is collaborative (vs unilateral) and proactive (vs reactive). Research continues to find that that the model is effective at not only solving problems and improving behaviour but also at enhancing adaptive communication and emotion regulation skills.
The Attachment Project is a (for profit) organisation that has useful Self-Help information for parents & caregivers (such as the specific link above) to help better understand how the different attachment styles develop in response to specific parenting strategies and styles. Their content is written by psychologists.
However, they offer an Attachment Style ‘quiz’ that is not a reputable diagnostic tool, nor is it empirically-validated (if you take this quiz, do so with ‘a grain of salt’). To their credit, the do state “The Attachment Project’s content and courses are for informational and educational purposes only. Our website and products are not intended to be a substitute for professional medical and/or psychological advice, diagnosis, or treatment.”
Summary:
Attachment science explains how humans develop and function in relationships across the lifespan.
Our ‘Attachment Style’ relates to the quality of our relationships with our primary caregivers.
Our earliest attachments with parents or caregivers shape our abilities and expectations for relationships throughout life. The quality of our bond within these early relationships influences how our sense of Self develops, what we expect from our partners, and how we believe relationships work.
Our early attachment experiences influence: How our brains developed; how we learned regulate our emotions in response to stress; and, how we relate to others and ourselves (including the partners we choose and how we believe relationships work, and we behave in relationships).
Attachment styles are not our fault (or our choosing). Rather, they emerge early in our lives and are the result of previously ADAPTIVE, self-protective (i.e., ‘survival’) behaviours, that we developed in response to our upbringing. These patterns are often carried forward into adulthood, even though the resulting effects on our relationships with ourselves and others may be compromised or may become ultimately unworkable.
Parents do not necessarily have to be highly abusive to have a negative effect on their children. Parents who are over-protective and intrusive, who are judgmental and have high expectations, or who are dismissive of a child’s thoughts and feelings can also cause a distrust of relationships – or even a distrust of a child’s own emotions – well into adulthood for that child.
Attachment in conjunction with adverse childhood experiences and other developmental deficits (resulting in difficulties with emotion regulation or maladaptive coping strategies), can lead to difficulties with emotion regulation in adults (such as a reduced Window of Tolerance).
Healing our attachment wounds is possible through a combination of learning, self-reflection, and heathy ’emotionally corrective relationships’ – this includes therapy with a trauma-informed, attachment aware therapist with whom you feel safe, understood and respected.
Although self-help information can be useful, there is a need for safe guided reflection and learning of interpersonal skills that cannot be mastered alone.
Because attachment is relational, we need an emotionally-attuned and emotionally-safe therapeutic environment in which to do this work. It involves working with our emotional understanding and responses in the context of interactions with others.
Therapies such as EMDR Therapy may be useful in helping you to remove the disturbance of painful memories so that you can put your past behind you, and create the relationships with yourself and others that you ultimately were unable to have. Regardless of the therapy ‘type’, ensure you seek the help of a therapist who is trauma-informed, and attachment aware.
Help for parents abounds in terms of individual and family therapy, and research-backed programs mentioned above in this article.
Couples with attachment difficulties are recommended to invest in therapy with a therapist who is trained in Emotionally Focused Therapy (EFT) for Couples. Based on attachment science, EFT is the gold standard for couples therapy a therapy. EFT for Couples not only addresses factors such as relationship distress, intimacy, trust, and the forgiveness of injuries, but it also aims to influence and heal you and your partner’s attachment style.
Understand that your attachment style may also affect how you engage in therapy. If you are receiving (or are planning to receive) therapy, I recommend reading the following article: How to get the most out of therapy.
I am a PhD Clinical Psychologist and EMDR Accredited Practitioner with over 15 years of psychotherapy experience. Whether you are seeking an assessment and diagnosis, or are searching for integrative research-backed ways to help you heal past wounds, break reactive-patterns and achieve long-lasting change, my aim is to provide a safe space for you to feel seen, understood, and empowered so you can make meaningful progress on your healing journey.
I endeavor to reply to all enquiries within 24 hrs.
About Me:
Dr Andreas Comninos, PhD Clinical Psychologist
I am a PhD Clinical Psychologist and EMDR Accredited Practitioner with over 15 years of psychotherapy experience. Whether you are seeking an assessment and diagnosis, or are searching for integrative research-backed ways to help you heal past wounds, break reactive-patterns and achieve long-lasting change, my aim is to provide a safe space for you to feel seen, understood, and empowered so you can make meaningful progress on your healing journey.
Adverse Childhood Experiences (ACEs) are traumatic events that happen early in life (childbirth to 18 years of age) that affect children while growing up, such as suffering maltreatment or living in a household affected by domestic violence, substance misuse or mental illness. Unlike single incident traumas, ACEs are often likely to last longer (or they may be repeated) and this can cause a child’s developing brain to become stuck in a physiological state of ‘threat’. When this happens, this stress may “toxic” to their psychological and emotional development, and in turn may affect their overall health.
Adverse Childhood Experiences (ACE) Study
The Adverse Childhood Experiences (ACE) Study (by the USA’s Centre for Disease Control & Intervention & Kaiser Permanente) is one of the world’s largest investigations of the effects of childhood abuse, neglect and household challenges on later-life health and well-being.
Completed in the late 1990s, 17,000 Kaiser patients completed a 10-question questionnaire (below) regarding their childhood experiences, and their current health status and lifestyle behaviours. Their answers were compared against their medical histories, and researchers were able to calculate with a high degree of accuracy, the relationship between ACEs and the likelihood of later medical issues.
Results from the study were shockingly clear: Early adversity can many have lasting impacts, including having a strong association with risky behaviours, susceptibility to mental health and chronic health conditions. Sadly, ACEs have a dose–response relationship, meaning the more ACEs an individual is exposed to, the greater the likelihood their health will be negatively impacted. However, keep in mind, that the people surveyed in the ACEs study, were not necessarily people who were actively engaged in treatment.
We know that the more ACEs children experience, the more harm they can sustain over time. In fact, we know that adults who have experiences one or more ACEs are at a higher risk for depression, diabetes, cancers, heart disease and other health conditions during their lifetime. For adults who have more than 4 ACEs and who have not received adequate therapy, this can negatively affect longevity through the role of unhelpful coping behaviours and negative lifestyle factors.
Examples of ACEs:
ACEs can increase risk of:
Child neglect (emotional, physical)
Parent or household mental illness
Parent or household substance use/alcoholism
Witnessing domestic violence
Having a parent or family member in jail
Parent separation or divorce
Death of a parent or sibling
Child abuse (emotional, physical, sexual)
Depression & other Mental Health issues
Alcoholism, Smoking
Teen pregnancy
Illicit drug use / Misuse of prescription drugs
Heart disease / Liver disease
Intimate partner violence
Sexually transmitted infections (STIs)
Suicide attempts / death by suicide
We now know that the more ACEs children experience, the more harm they can sustain over time. In fact, we know that adults who have experienced one or more ACEs as a child are at higher risk of depression, cancer, heart disease, diabetes and other health conditions during their lifetime. For adults who have experienced over four or more ACEs and who have not received adequate therapy, this can even negatively affect longevity through the role of unhelpful coping behaviours and negative lifestyle factors.
Unfortunately, Parents who have experienced ACEs and who have not developed adaptive ways to resolve the complex and challenging impacts of these experiences, or who may have not have developed adaptive ways of coping with stress, are (sadly) statistically more likely to create environments – or have lifestyles – that place their offspring at risk of experiencing ACEs themselves. Often, this is how the cycle of inter-generational trauma continues.
Below is an animation illustrating how ACEs develop and may be passed on intergenerationally:
The ACE Questionnaire:
To determine someone’s ACEs score, they answer the 10 Adverse Childhood Experiences questions relating to events prior to their eighteenth birthday:
Did a parent or other adult in the household often or very often… Swear at you, insult you, put you down, or humiliate you? or act in a way that made you afraid that you might be physically hurt?
Did a parent or other adult in the household often or very often… Push, grab, slap, or throw something at you? or Ever hit you so hard that you had marks or were injured?
Did an adult or person at least 5 years older than you ever… Touch or fondle you or have you touch their body in a sexual way? or Attempt or actually have oral, anal, or vaginal intercourse with you?
Did you often or very often feel that … No one in your family loved you or thought you were important or special? or Your family didn’t look out for each other, feel close to each other, or support each other?
Did you often or very often feel that … You didn’t have enough to eat, had to wear dirty clothes, and had no one to protect you? or Your parents were too drunk or high to take care of you or take you to the doctor if you needed it?
Were your parents ever separated or divorced?
Was your parent or caretaker: Often or very often pushed, grabbed, slapped, or had something thrown at her? or Sometimes, often, or very often kicked, bitten, hit with a fist, or hit with something hard? or Ever repeatedly hit over at least a few minutes or threatened with a gun or knife?
Did you live with anyone who was a problem drinker or alcoholic, or who used street drugs?
Was a household member depressed or mentally ill, or did a household member attempt suicide?
Did a household member go to prison?
Toxic Stress and ACEs
In addition to the hugely influential nature of the Attachment relationship between a parent and a child, ongoing adverse experiences (such as those listed above) can cause toxic levels of stress that sadly can negatively impact on both brain structure (i.e., the development of neural networks) and brain function (i.e., can alter a developing brain’s biochemistry and thus response to input).
Toxic stress happens when ACEs repeatedly trigger a child’s fight-flight-freeze system (our innate stress response governed by our sympathetic nervous system). It also occurs when emotions associated with coping (like anger, fear, frustration, shame, humiliation, anxiety) continue to trigger a stress response in the body and mind. This is commonplace in families where children are either punished for their emotional experiences, or parents who may lack the skills / awareness to navigate certain emotions themselves miss opportunities (cues) to settle and soothe their children.
With repeated exposure to high levels of stress (particularly in the absence of attachment safety), the accumulation of toxic stress can affect both skill and brain development. Living an a heightened state characteristic of perpetual fear (or the need to ensure safety) can effectively narrow our Window of Tolerance making us susceptible to chronic health conditions.
Hopefully it is becoming clearer to you that the devastating impact of toxic stress on a developing brain (and the resulting emotion-regulation and skill deficits people are left with) is not the fault of the individual. Rather, it is the outcome of not having a safe and secure development. This results in a child missing many important skills and experiences that build resilience, or a child’s brain being negatively affected in ways that can become pervasive in later life.
As we develop, particularly in the absence of supportive caregivers or healthy role models, toxic stress may also lead to less-than-ideal coping behaviours that may negatively affect our health. Over time and into adulthood, these coping behaviours can in turn cause health effects that can accumulate across a lifetime.
Summary of Key Findings from 17,000+ patients in the CDC-Kaiser Study
Due to the now well-documented effects of long-term toxic stress, the higher your ACE score the more likely you are to emerge from childhood with emotional and/or behavioural difficulties that can affect the rest of your life. In other words, the higher your ACE score the higher your statistical chance of suffering from a range of psychological and medical problems like chronic depression, cancer, or coronary heart disease.
Key findings from the ACEs study are summarized below:
The original study us available in full (via an external link) here.
Alarmingly, we now know that people who do not heal from their traumas are more likely to raise children who go on to have high ACE scores. In other words,
Untreated childhood trauma becomes a source of Intergenerational Trauma
Thankfully, although the effects of toxic stress can be profound, they can be significantly lessened by protective factors that build resilience and can buffer the effects of trauma. We know that safe, stable, and nurturing relationships can protect our brains and bodies from the harmful effects of stress and adversity.
We also know that healthy nutrition, regular exercise, restful sleep, practicing mindfulness, building social connections, and getting mental health support can all help decrease toxic stress hormones associated with ACEs and can improve health.
10 Important Things to Know About Adverse Childhood Experiences
Below is Part 1 of a hugely informative (but easy to follow) 5-Part video series by Dr. Colleen Bridger that explores the impacts of Adverse Childhood Experiences (ACEs) on a child’s developing brain and how trauma can influence both emotional and behavioural expression.
It presents eye-opening examples of ways trauma can shut down (or can activate) a child’s nervous system and how behavioural problems in children can be easily mistaken (and misdiagnosed) particularly when a narrow symptom-focus that overlooks the impacts of ACEs is used.
Click the following links for the remaining parts to this talk:Part 2 | Part 3 | Part 4 | Part 5.
Problems with ACEs Study: Correlation is NOT Causal
The ACEs Study is essentially a ‘snapshot’ of people who had adverse childhood experiences and where they were at later in their lives. It is not possible to infer direct causation from this research (i.e., it is an over simplification to say ‘ACEs cause later difficulties’). Similarly, the Study did not look at whether or not participants had received any treatment for their traumas (or what kind). We know that trauma-informed therapies (like EMDR Therapy) can greatly help people to ‘get past their past’ which is especially important for people who are affected by ACEs.
Also, keep in mind that ACE Questionnaire is very brief and it is not exhaustive (after all, it is only 10 questions…). Because of this, it does not list all possible adverse events that can happen within a family situation. We also know that Attachment issues between a parent and a childcan also have a huge impact on the emotional development and learning that a child can carry with them through adulthood. Equally – so too can events that occur outside the home (e.g. bullying at school).
However – and this is important – the ACE questions do not ask about any protective factors. For example, we know that having a healthy relationship with at least one caring adult or parent, who is emotionally attuned to your emotional and developmental needs can make up for a non-secure (or absent, or abusive) relationship with another caregiver / parent.
Indeed, not everyone who experiences one or more ACEs will go on to developing a serious mental health or medical issue. In fact, many adults who experience significant adversity in their childhood have gone on to have amazing lives full of adventures, achievements, and happy relationships and families. This is because although the effects of toxic stress can be profound, they can be significantly lessened by protective factors that build resilience and can buffer the effects of trauma.
Again, we know that these adults have identified that this resilience was helped by having at least one healthy, safe, caring relationship in their life. This is because safe, stable, and nurturing relationships can protect our brains and bodies from the harmful effects of stress and adversity.
A safe, stable, and nurturing relationship can come from a number of different people – for instance, a different parent, sibling, relative, teacher, mentor, therapist, or coach.
A safe, stable, and nurturing relationship for a developing child is:
An emotionally responsive and a supportive person in their life (Someone they can lean on)
Someone who views them as unique and interesting (Someone who is interested in them)
Someone who supports their ideas or dreams (Someone who believes in them)
If you are a survivor of childhood trauma, it is recommended that you find a trauma-informed psychologist who can provide a securely attached, emotionally corrective relationship in which you can process your past, learn the emotional regulation and relationship skills that you may have missed out on, so that you can learn to break the patterns of your upbringing.
Equally, if you are a parent who has experienced ACES or you are the parent of a child who has experienced ACEs, it is equally important to seek professional help to mitigate the effects of this trauma.
Summary
Adverse Childhood Experiences (ACEs) are traumatic events that happen early in life (childbirth to 18 years of age), such as suffering maltreatment or living in a household affected by domestic violence, substance misuse or mental illness.
ACEs may cause a child’s developing brain to become stuck in a physiological state of ‘threat’.
This may affect a child’s brain development, and psychological functioning and this may influence lifestyle behaviours that affect overall long-term health.
Parents who have experienced ACEs are (sadly) statistically more likely to create environments – or have lifestyles – that place their offspring at risk of experiencing ACEs themselves. Often, this is how the cycle of inter-generational trauma continues.
ACEs are not causal (and the questionnaire does not measure ‘protective factors’)
Although the effects of toxic stress can be profound, they can be significantly lessened by protectivefactors that build resilience and can buffer the effects of trauma.
With the appropriate help, adults who experience significant adversity in their childhood can go on to have amazing lives full of adventures, achievements, and happy relationships and families.
Safe, stable, and nurturing relationships can protect our brains and bodies from the harmful effects of stress and adversity.
Healthy nutrition, regular exercise, restful sleep, practicing mindfulness, building social connections, and getting mental health support can also help decrease toxic stress hormones associated with ACEs and can improve health.
I am a PhD Clinical Psychologist and EMDR Accredited Practitioner with over 15 years of psychotherapy experience. Whether you are seeking an assessment and diagnosis, or are searching for integrative research-backed ways to help you heal past wounds, break reactive-patterns and achieve long-lasting change, my aim is to provide a safe space for you to feel seen, understood, and empowered so you can make meaningful progress on your healing journey.
I endeavor to reply to all enquiries within 24 hrs.
About Me:
Dr Andreas Comninos, PhD Clinical Psychologist
I am a PhD Clinical Psychologist and EMDR Accredited Practitioner with over 15 years of psychotherapy experience. Whether you are seeking an assessment and diagnosis, or are searching for integrative research-backed ways to help you heal past wounds, break reactive-patterns and achieve long-lasting change, my aim is to provide a safe space for you to feel seen, understood, and empowered so you can make meaningful progress on your healing journey.